

How to Properly Document Medical Necessity for Personal Injury Insurance Claims?
Documenting medical necessity for personal injury insurance claims means proving every service was safe, effective, appropriate for the diagnosis, and not experimental. That proof lives in your SOAP notes and every attachment you send. It's not a box to check. It's a story you're telling to someone who already doubts you.
The adjuster reads for gaps. Missing information is one of the most frequent reasons claims get denied. Every procedure must link to a specific diagnosis code. Every visit note must include the patient's subjective experience, your objective findings, your assessment, and your plan. If any piece is missing, the claim is vulnerable.
Medical necessity documentation for PI claims isn't about writing more. It's about writing defensibly.
The question isn't whether your patient needed care. The question is whether you can prove it on paper, under scrutiny, months after the visit. That documentation either holds or it doesn't. Most practices don't realize it's broken until the settlement check is smaller than expected. Or until the lien gets devalued because the records couldn't defend themselves.
Proper documentation starts with knowing what the adjuster is looking for. They need to see the care was reasonable and necessary. They need to see progression. They need to see you linked every service to a diagnosis. And they need to see the clinical story matches the billing. If those pieces aren't there, the claim won't survive scrutiny.
Last Updated: May 23, 2026
- What Medical Necessity Means in Personal Injury Claims
- The Core Components of Medical Necessity Documentation
- Where Most Practices Lose Revenue on Documentation Failures
- How to Write a Medical Necessity Letter That Defends Your Care
-
Frequently Asked Questions
- What are the absolute essential components of a medical necessity letter for a PI claim?
- How do SOAP notes for a personal injury case differ from those for a standard insurance claim?
- What are the most common documentation mistakes that cause PI claims to be denied or devalued?
- Can I use an EHR template for medical necessity documentation in a PI case, or does it need to be customized?
- How often should I be documenting progress to sufficiently establish medical necessity over the course of care?
- The Documentation Standard That Protects Your Revenue
What Medical Necessity Means in Personal Injury Claims
Here's the problem with most explanations of medical necessity: they're technically correct and completely useless.
You don't need a definition. You need to know what the insurance industry will actually accept — and what happens when your documentation doesn't match that standard.
Medicare sets the official definition of medical necessity that most insurance companies follow, even in personal injury claims. A service is medically necessary if it's safe and effective, not experimental or investigational, and appropriate for the patient's illness or injury.
That's the threshold. If your documentation doesn't prove all three criteria, the claim is at risk. Not flagged for review — at risk of being denied or devalued outright.
The Three-Part Standard
Safe and effective means the treatment has documented clinical support.
It's not enough to say you adjusted the patient. Your notes need to document what you found on examination and why that adjustment was the clinically appropriate response to those findings.
Not experimental or investigational means the treatment is recognized as standard care for the diagnosis you're treating.
If you're using a modality that's outside mainstream chiropractic practice, you'll need extra documentation to defend it. That doesn't mean you can't use it — it means you can't assume the payer will accept it without explanation.
Appropriate for the diagnosis means every service maps directly to a diagnosis code that justifies it.
You can't bill for lumbar manipulation if your diagnosis is cervical radiculopathy. The clinical story has to match the codes. And the codes have to match the story. Both directions.
Why PI Claims Get Held to a Higher Standard
Personal injury claims get scrutinized harder than standard insurance billing.
Standard claims get processed by automated systems that check for basic compliance. PI claims get reviewed by adjusters and attorneys who are actively looking for reasons to reduce what they owe. That's not cynicism — it's their job.
The stakes are higher.
A standard insurance claim might be worth a few hundred dollars. A PI lien can represent months of care and thousands of dollars in deferred revenue. That difference changes how the payer reads your documentation — and how aggressively they'll challenge it.
And the timeline is longer.
Standard claims get adjudicated within weeks. PI claims sit for months — sometimes over a year — before settlement. By the time someone reads your notes, the case is cold. Your documentation has to tell the full story without you there to explain it.
If it does not, you lose negotiating power at the settlement table. That's where most practices find out their records were not strong enough to defend how to file a chiropractic lien.
The Core Components of Medical Necessity Documentation
So what actually goes in the records?
Not the generic stuff. The PI-specific pieces that hold up under scrutiny.
Three things have to be in every PI record: a complete SOAP note structure, a clear link between every treatment and its diagnosis code, and consistent progress documentation that shows whether the patient is improving.
These aren't separate tasks. They're the same clinical story told three different ways.
Miss one, and the entire case weakens.
The SOAP Note Structure
The structure of a SOAP note is the foundation.
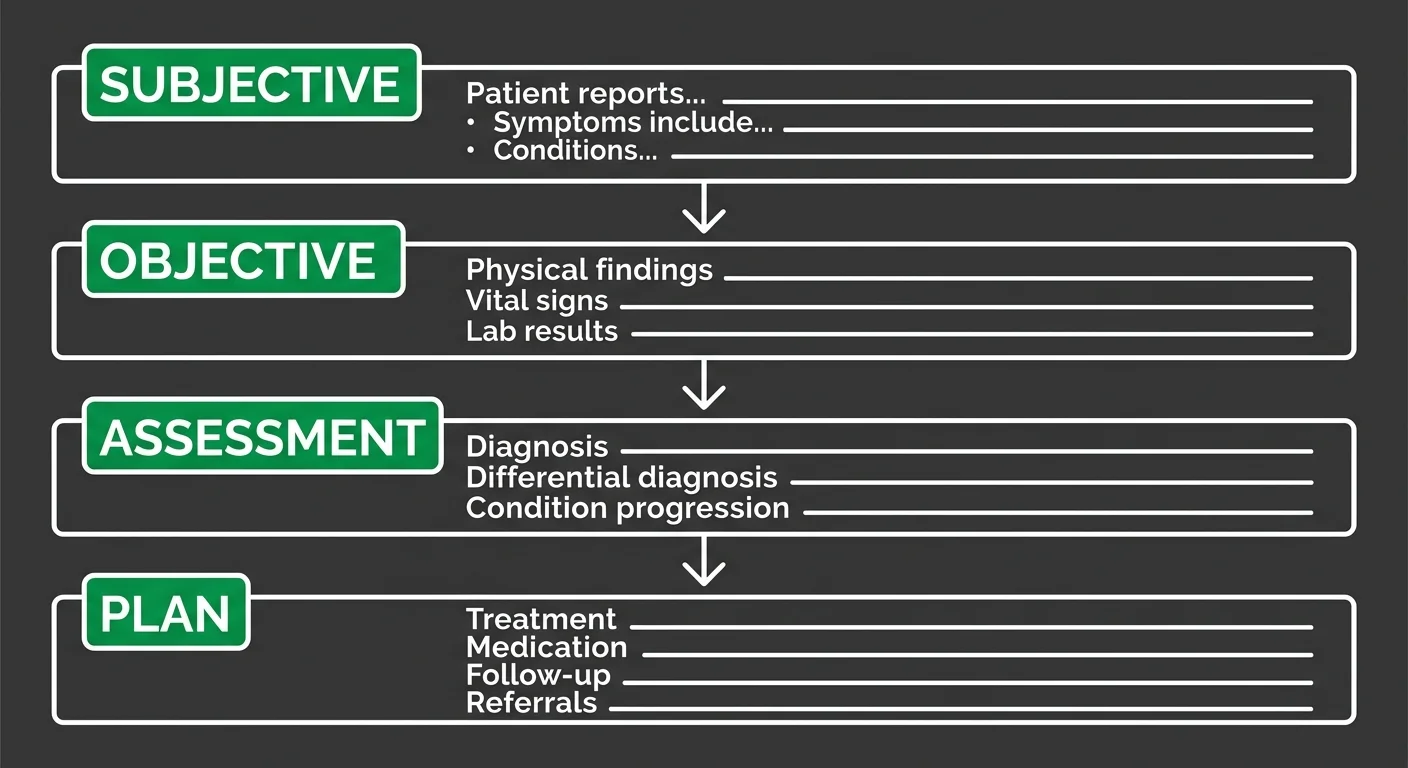
Subjective, Objective, Assessment, Plan — those four sections live in every visit note. No exceptions.
The Subjective section captures what the patient reports — pain level, location, what makes it worse. The Objective section records what you find — range of motion, palpation findings, orthopedic tests. The Assessment section names the diagnosis. The Plan section documents the treatment you delivered and what you're doing next.
Each section answers a specific question the adjuster will ask months from now when they're deciding what your lien is worth.
But generic SOAP templates don't cut it in PI cases.
Chiropractic practices need chiropractic-specific documentation standards that address manipulation and manual therapy billing. Insurance adjusters expect clinical detail that general templates don't capture.
The American Chiropractic Association's Clinical Documentation Manual provides the specialty-level guidance that makes records defensible in legal and insurance contexts.
Linking Treatment to Diagnosis
Every procedure code you bill must map to a diagnosis code that justifies it.
That's the mechanism that proves medical necessity. Not optional.
Billing lumbar manipulation? The diagnosis needs to support lumbar treatment.
Billing cervical manipulation? The diagnosis needs to justify cervical care.
The codes have to match the clinical story. And the clinical story has to match the patient's documented presentation. Insurance adjusters hunt for disconnects — where the diagnosis doesn't support the service, or where the service doesn't align with the findings.
Here's where practices lose money.
They bill correctly. They document care. But they don't link the two tightly enough to survive review months later when an attorney reads the file.
If the connection isn't explicit in the record, the adjuster assumes it isn't there. And if it isn't there, the claim gets devalued.
Progress Documentation
Progress documentation shows whether the care is working.
Every adjuster asks: is the patient improving, plateauing, or worsening?
If your notes don't track progression, the claim looks like maintenance care. And maintenance care isn't medically necessary.
You need measurable data points at regular intervals — pain scales, functional assessments, range of motion changes.
You need to document when the patient's condition improves and when it doesn't. And you need to explain why you're continuing care if progress has plateaued.
Without that narrative, the documentation tells a story of overutilization instead of medical necessity. That's the story the adjuster uses to reduce your lien.
| SOAP Component | What It Documents | Why It Matters for PI Claims |
|---|---|---|
| Subjective | The patient's reported experience — pain level, functional limitations, symptom changes, how they're responding to care | Proves the patient's complaints are consistent with the claimed injury and establishes the baseline severity that justifies treatment intensity |
| Objective | Provider's clinical findings — range of motion measurements, orthopedic test results, palpation findings, observable postural or gait abnormalities | Provides measurable, verifiable evidence that the injury exists and supports the diagnosis — the adjuster can't argue with documented findings |
| Assessment | The clinical diagnosis tied to specific ICD-10 codes that justify the treatments billed | Links every service to a medically necessary reason — without this connection, the claim looks like unbillable maintenance care |
| Plan | The proposed treatment, frequency, duration, and clinical reasoning for why this specific approach is appropriate for the diagnosis | Demonstrates that care is goal-oriented and not open-ended — shows the adjuster you're treating toward resolution, not perpetuating visits |
Where Most Practices Lose Revenue on Documentation Failures
The mistakes that cost practices the most aren't the ones that get claims denied outright.
They're the ones that quietly devalue liens and settle for less than the care was worth.
Most practices don't lose revenue because they documented nothing. They lose it because they documented incompletely.
The gaps aren't obvious when you're writing the notes. They're obvious months later when an adjuster is looking for a reason to reduce the settlement.
By then, you can't fix it. The record is closed. And the revenue is gone.
Missing or Incomplete Information
Missing or incomplete information is one of the most frequent reasons for claim denials. Not because the care wasn't necessary.
Because the record doesn't prove it was.
A SOAP note missing the Objective section leaves the adjuster guessing whether you actually examined the patient. A Plan that doesn't explain why you're continuing care reads as maintenance. An Assessment that lists a diagnosis code without connecting it to your findings makes the treatment look arbitrary.
Every gap creates doubt.
Doubt reduces what the claim is worth.
The American Medical Association reports that common reasons for claim denials frequently include missing information that directly impacts the ability to prove medical necessity.
The claim might get paid. But it'll get paid less.
The adjuster sees incomplete documentation as a tool to negotiate down. That's where practices lose money — not in full denials, but in quiet devaluations they don't see coming.
Using EHR Templates Without Customization
EHR templates are built for speed. They're designed to help you document quickly and move to the next patient.
But PI claims don't get adjudicated quickly. They get scrutinized slowly.
And generic templates don't hold up under that scrutiny.
A template that auto-populates 'patient tolerated treatment well' every visit tells the adjuster nothing about whether the patient actually improved. A template using the same Objective findings week after week makes it look like you didn't examine the patient.
A template that doesn't customize the Plan to reflect changing clinical findings makes the care look routine instead of medically necessary.
Templates work for standard insurance billing because those claims get processed by software checking for basic compliance. PI claims get read by people trained to spot patterns that suggest overutilization or lack of individualized care.
If your notes look identical visit to visit, the adjuster assumes the care was identical visit to visit.
That assumption costs you at settlement. This is part of why PI liens take longer to settle — and why the documentation has to be stronger than what works for standard billing.
Failing to Document the Patient's Functional Limitations
Pain levels matter. But functional limitations matter more.
An adjuster reading your notes six months after the accident doesn't care that the patient reported 7/10 pain. They care whether the patient could sit through a work shift, lift their kids, or sleep through the night.
Functional documentation proves impact. It shows that the injury affected the patient's life in measurable ways. It shows that your care restored function.
And it shows that without your care, the patient's condition would've worsened or plateaued.
That's the narrative that justifies the lien amount.
Practices that document pain without documenting function leave money on the table.
The settlement negotiator doesn't need to prove your care wasn't necessary. They just need to prove your records don't show it was.
If the functional story isn't in the documentation, it doesn't exist. And if it doesn't exist, the lien gets reduced.
| Documentation Failure | What Gets Lost | Revenue Impact |
|---|---|---|
| Identical SOAP notes visit to visit | Evidence of individualized clinical judgment | Adjuster assumes templated care rather than medically necessary treatment — settlement offer reduced without explanation |
| Missing Objective findings in progress notes | Proof that the patient was actually examined | Claim appears unsupported by clinical findings — lien value questioned during settlement negotiation |
| No documented functional limitations | Evidence of real-world impact and recovery | Settlement negotiator argues care wasn't necessary because records don't show measurable functional improvement |
| Diagnosis codes that don't match billed procedures | The link proving medical necessity | Services get unbundled or denied as not medically necessary — practice absorbs write-offs months after care concluded |
| No explanation for continued care after plateau | Clinical rationale for treatment duration | Entire treatment phase gets reclassified as maintenance — practice receives fraction of billed amount at settlement |
How to Write a Medical Necessity Letter That Defends Your Care
When a claim is challenged or a lien is disputed, the medical necessity letter is your last line of defense. It's where most practices either win or fold.
The letter isn't a summary of care. It's an argument.
You're defending the clinical decision-making that justified every visit, every procedure, and every dollar on the lien. The adjuster or attorney reading it isn't looking for confirmation. They're looking for gaps.
If your letter doesn't anticipate their objections and address them directly, it won't hold. And if it doesn't hold, the lien gets reduced or denied. That's the moment when incomplete documentation from months earlier becomes a revenue problem you can't fix.
The Structure of the Letter
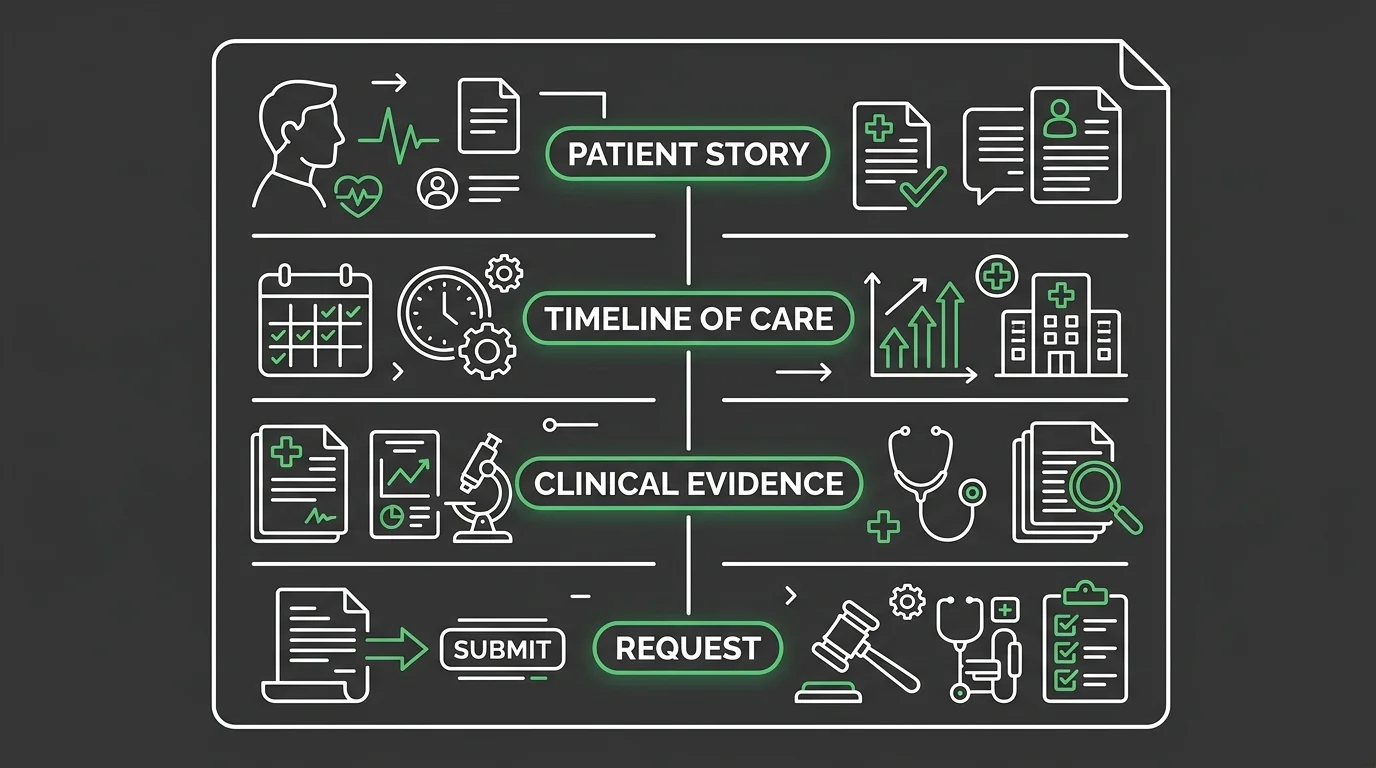
Writing an effective appeal letter requires four components: the patient's story, a timeline of care, clinical evidence supporting the treatment, and a clear statement of what is being requested.
Those four components aren't optional. They're the structure that makes the letter defensible.
Miss one, and the argument collapses.
The patient's story establishes context. What happened in the accident? What was the presenting condition? Why was immediate intervention necessary?
The timeline of care shows progression. When treatment started. How often they were seen. When their condition improved. When care was reduced or discharged.
The clinical evidence ties your documented findings to the services you provided. The request is what you're asking for — reinstatement of the claim, payment of the full lien amount, reconsideration of the denial.
This structure is built specifically for situations where medical necessity is being questioned. The letter has to tell a complete story that can stand alone without the adjuster needing to reread your entire patient file.
If they have to hunt for the justification, they won't. They'll just reduce the claim.
What to Include in Each Section
Each section of the letter serves a specific defensive function. The patient's story isn't filler. It's the foundation that makes the rest of the argument credible.
Document the mechanism of injury. Document the patient's initial presentation. Document the functional limitations they reported at the start of care.
You're showing the injury was significant enough to require intervention. You're establishing baseline.
Without that context, the adjuster reads your treatment plan as aggressive. With it, they see the care as responsive to a documented clinical problem.
The timeline section prevents the adjuster from misinterpreting the frequency or duration of care. Walk them through when the patient was seen. Why the frequency was appropriate at each phase. When the treatment plan was modified based on clinical progress.
Connect every change in the care plan to a documented change in the patient's condition.
That's how you prove the care wasn't routine. It was individualized and medically necessary.
The clinical evidence section is where you cite your documentation directly. You're pulling specific SOAP note findings — range of motion measurements, orthopedic test results, functional assessments — and showing how they justified the procedures you billed.
You're referencing state-specific medical records laws where applicable to show your documentation meets legal standards. You're not summarizing. You're quoting your own records to prove the treatment was supported by objective clinical findings at every visit.
That's what separates a letter that holds from one that folds under scrutiny.
| Letter Section | Purpose | Key Elements to Include |
|---|---|---|
| Patient Story | Establishes clinical context and injury severity | Mechanism of injury, initial presentation, baseline functional limitations, chief complaint, and why immediate intervention was necessary |
| Timeline of Care | Demonstrates that care frequency and duration were responsive to clinical need, not arbitrary | Start date, visit frequency at each phase, when condition improved, when treatment plan was modified, and when care was reduced or discharged |
| Clinical Evidence | Proves that every billed service was justified by documented objective findings | Specific SOAP note findings (ROM measurements, orthopedic tests, functional assessments), quotes from your own records, and citations showing how findings supported procedures |
| Request | Clearly states what you're asking the adjuster or payer to do | Specific action requested (reinstatement of claim, payment of full lien amount, reconsideration of denial), dollar amount if applicable, and deadline for response |
Frequently Asked Questions
These questions show up after the damage is done.
After the lien gets reduced. After the settlement negotiator pushes back. After the adjuster requests more records and you realize your notes don't answer what they're actually asking.
Here's what protects revenue when the documentation is under scrutiny.
What are the absolute essential components of a medical necessity letter for a PI claim?
A medical necessity letter for a PI claim needs four core elements.
The patient's story — the accident mechanism, initial presentation, and baseline functional limitations. This establishes causation.
A timeline showing when treatment started, how often the patient was seen, and when care was modified. This proves the treatment wasn't static.
Clinical evidence that ties your documented findings to the services you billed. This defends the procedures.
And a clear request — reinstatement, full payment, or reconsideration. This tells the adjuster what you want.
Miss any one of those, and the letter won't hold. The adjuster won't hunt for the missing piece. They'll just reduce the claim.
How do SOAP notes for a personal injury case differ from those for a standard insurance claim?
PI SOAP notes have to prove causation and progression in ways standard claims don't.
The Subjective section documents the patient's experience. But for PI you're also tracking mechanism of injury and functional limitations over time — not just pain.
The Objective section records your findings. You're including orthopedic tests and range-of-motion measurements that tie directly to the accident — not generic exam findings.
The Assessment establishes the diagnosis. The Plan outlines treatment. Both have to show individualized decision-making, not template care.
Standard claims get paid if the diagnosis code matches. PI claims get paid if the narrative holds.
What are the most common documentation mistakes that cause PI claims to be denied or devalued?
Missing or incomplete information is one of the most frequent reasons for claim denials.
Practices leave gaps that insurance adjusters exploit.
They don't link every service to a diagnosis code. The adjuster questions medical necessity.
They document pain levels without documenting functional limitations. The settlement negotiator can't see the impact.
They use template notes that don't reflect individualized care. The lien gets devalued as routine maintenance.
Every one of those mistakes is preventable. But only if you're building the documentation with scrutiny in mind.
Can I use an EHR template for medical necessity documentation in a PI case, or does it need to be customized?
EHR templates work for standard claims. They don't work for PI cases.
Templates generate notes that look identical visit to visit. That's a red flag for adjusters reviewing the lien. They read templated documentation as routine care, not individualized treatment.
You need to customize the notes to reflect what actually changed at each visit.
That means editing the Subjective section to capture the patient's functional progress.
That means updating the Objective findings to show clinical improvement or plateau.
That means modifying the Plan to show why you adjusted frequency or introduced new procedures.
If your notes could've been written by a macro, they won't defend your revenue.
How often should I be documenting progress to sufficiently establish medical necessity over the course of care?
You should be documenting progress at every visit. Not summarizing it at discharge.
Every SOAP note needs to show what changed since the last visit. Range of motion improved. Pain levels decreased. Functional limitations resolved. Orthopedic tests normalized.
That's how you prove the care wasn't static.
Adjusters reviewing the lien months later are looking for progression. If your notes don't show it visit by visit, they can't see it at all.
And if they can't see it, they assume it didn't happen. That's when the lien gets reduced.
The Documentation Standard That Protects Your Revenue
Documentation isn't about whether you provided good care.
It's about whether you can prove it when someone's paid to doubt you.
The adjuster reviewing your lien isn't looking for reasons to approve it. They're hunting gaps. The insurance attorney reading your notes isn't assuming medical necessity. They're building the argument that your care was excessive. The settlement negotiator isn't honoring the clinical value of your services. They're calculating how low you'll go.
Your documentation is the only thing standing between you and all three.
And if it can't tell the story clearly, completely, and convincingly — you lose revenue you'll never see again.
Medical necessity documentation for PI claims isn't a compliance task. It's a story you're telling to someone who's already decided you're exaggerating.
The question isn't whether your patient needed care. The question is whether you can prove it on paper, under hostile review, six months after the case closed.
That story either survives scrutiny or it collapses.
Most practices don't know it collapsed until the settlement check comes in lower than expected — or until the lien gets slashed because the documentation couldn't defend the billing.
The practices that protect their revenue document like they're preparing for deposition. Every service maps to a diagnosis. Every visit tracks measurable functional change. Every note reflects individualized clinical judgment. Every medical necessity letter anticipates the objections before the adjuster raises them.
They don't wait for a reduction notice to realize the documentation was thin.
They build the clinical argument in real time — while the patient is still under care.
This is where automation-forward billing companies structurally abandon revenue.
Volume-first models optimize for claim submission speed. They don't budget time for medical necessity arguments. They don't prioritize human review of clinical narratives. And they don't fight for liens that require more than a template and a procedure code.
When the documentation requires a nuanced defense, the claim gets written off.
The practice assumes the biller is working it. The biller assumes the documentation won't hold up. And the revenue vanishes without a conversation.
Bushido Billing was founded by someone who ran a chiropractic practice and knows exactly what weak documentation costs. We don't treat PI liens like data entry. We treat them like the clinical arguments they are.
We review your notes before the lien is filed. We flag gaps while you can still strengthen them. And when a lien gets challenged, we write the medical necessity defense that protects your revenue — because we get paid when you do.
If your current billing partner treats PI documentation like a submission checklist instead of a legal defense document, you're losing money every time a lien settles for less than it should.
If your billing company treats PI documentation like a submission requirement instead of a defense strategy, you're losing money every time a lien settles. You built the clinical case. Someone has to defend it when the adjuster pushes back. See where your documentation is costing you — and what it takes to recover what you're leaving on the table.

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet