

Human Intelligence vs. AI Coding: Which One Prevents Audits in a High-Specificity Market?
Auto-coders submit claims. They do not defend them. That distinction is the entire audit problem for chiropractic practices in 2026.
Automated EHR coding platforms apply codes based on templated logic and push submissions out fast. What they cannot do is evaluate whether the clinical documentation behind those codes satisfies the medical necessity standards auditors actually examine.
Chiropractic billing runs on documentation requirements that are specific, non-negotiable, and under active federal scrutiny. The AT modifier must be appended to Medicare chiropractic claims to distinguish acute therapeutic spinal manipulation from non-covered maintenance care. An auto-coder can apply that modifier. It cannot assess whether the underlying clinical notes substantiate it.
That is exactly where audits find their footing.
The OIG has identified chiropractic claims as a high-error category, with prior reviews documenting error rates tied directly to failures in proving active treatment through correct documentation. The pattern repeats every audit cycle: claims go out, modifiers get applied, and when a reviewer examines the actual notes, the documentation doesn't hold up.
That is not a technology failure. It is a judgment failure. And judgment is not something any algorithm currently supplies.
The 2026 ICD-10 updates add another layer. ICD-10-CM categories Z55 through Z65 now document Social Determinants of Health — clinical variables tied to socioeconomics and environmental factors that affect how conditions are coded and how medical necessity is established. A templated auto-coder was not built to interpret those categories in a chiropractic context.
Peer-reviewed research confirms that clinical documentation quality in alternative medicine settings improves when human review protocols replace automated templates. Human reviewers catch contextual errors that rule-based systems miss.
Submitting a claim and defending a claim are two entirely different jobs. In a high-specificity specialty market, only one of them determines whether a practice survives an audit. And only one of them requires human clinical intelligence.
Last Updated: June 22, 2026
- • Why Chiropractic Is the Highest-Audit-Risk Specialty in Medicare
- • Why Auto-Coders Were Never Built for Chiropractic Specificity
- • What the 2026 ICD-10 SDOH and Medicare Updates Actually Require
- • What Human Clinical Intelligence Does That Algorithms Cannot
- • How to Evaluate Whether Your Current Coding Is Audit-Ready
-
• Frequently Asked Questions
- • How do automated EHR coding tools increase chiropractic audit risk?
- • Why can't AI coding tools distinguish active therapeutic care from maintenance care?
- • How do the 2026 ICD-10 SDOH updates affect chiropractic claim audits?
- • What does it actually cost a practice when an auto-coder fails during a Medicare audit?
- • How does an embedded human billing partner defend coding specificity that software cannot?
- • Is a DC-founded billing company actually better positioned to handle these audits?
- • The Verdict: Detection Is Not Defense
Why Chiropractic Is the Highest-Audit-Risk Specialty in Medicare
Chiropractic isn't randomly targeted. It earns its place at the top of Medicare's audit list. The specialty carries documentation requirements that are structurally different from every other provider type — and those differences create predictable failure points that repeat every audit cycle.
The core exposure is the active versus maintenance care distinction. Medicare covers spinal manipulation only when it's clinically necessary and actively therapeutic. That determination lives in the clinical documentation — not the code, not the modifier, not the software platform. Documentation is where chiropractic practices are most exposed. And documentation is exactly where automated systems fall short.
This isn't a gray area. Chiropractic sits in a high-priority target zone — and the practices that underestimate that reality are the ones writing checks to audit recovery firms.
The OIG's Sustained Focus on Chiropractic Claims
The OIG has maintained sustained attention on chiropractic Medicare claims for years. Prior reviews documented extensive error rates tied directly to failures in proving active treatment through correct documentation. The OIG's pattern isn't about fraud. It's about documentation that can't hold up under review — claims submitted in good faith, built on clinical notes that don't satisfy what an auditor is actually checking for.
That distinction matters more than most practices realize. A practice can bill in complete good faith and still fail an audit — because the clinical notes don't adequately establish that care met Medicare's definition of active therapeutic treatment. NIH research into clinical documentation quality confirms these gaps are consistent and systemic. They're not isolated errors. They're structural.
The OIG doesn't move on from chiropractic. It returns — because the error patterns return. The 2026 regulatory cycle compounds the documentation complexity further. Practices that haven't addressed these structural vulnerabilities are walking into the next review cycle carrying the same exposure they had in the last one. The first step toward building a defensible position is understanding the full scope.
Why Generic Billing Practices Trigger Chiropractic-Specific Flags
Generic billing fails chiropractic because it applies general medical logic to a specialty with non-general rules. The AT modifier is the clearest example. It isn't a universal billing concept. It's a chiropractic-specific Medicare requirement — and applying it correctly depends on understanding what it's defending and why auditors check it.
A generalist approach — whether human or automated — treats the AT modifier as a checkbox. A chiropractic-specific approach treats it as a clinical argument that the underlying notes either support or don't. Published analysis on Medicare chiropractic billing requirements makes clear that this is where most audit failures originate. The claim isn't the problem. The documentation behind the claim is.
That's exactly why chiropractic billing services built for this specialty operate differently than generalist services that happen to include chiropractic in a dropdown menu. Specialty-level billing means someone is reviewing clinical notes against the modifier being claimed — every time, not just when an audit notice arrives. The review isn't reactive. It's structural.
| Audit Risk Factor | Why It Applies to Chiropractic | What Auditors Look For |
|---|---|---|
| Active vs. Maintenance Care Distinction | Medicare only covers spinal manipulation that is actively therapeutic — not care that maintains a patient's current condition. Chiropractic is the only specialty where this line is drawn explicitly in coverage policy, making every claim a documentation argument about clinical necessity. | Whether the clinical notes establish that treatment was actively improving the patient's condition at the time of service — not simply maintaining function or managing chronic symptoms. |
| AT Modifier Requirement | The Active Treatment modifier must appear on every covered Medicare chiropractic claim. It is a chiropractic-specific requirement with no direct equivalent in most other specialties. Its presence signals acute care eligibility — but auditors verify that the underlying documentation supports that signal. | Whether the modifier is applied correctly and whether the clinical record substantiates it. A modifier without supporting documentation is treated as a red flag, not a technicality. |
| Sustained OIG Oversight Focus | Chiropractic has remained a recurring subject of federal oversight reviews because error patterns tied to documentation failures have appeared consistently across review cycles. The OIG does not move on from a specialty until the error patterns stop recurring. | Whether documentation practices have changed since prior review findings — and whether the same failure modes that triggered past error rates are still present in current claim submissions. |
| Complexity of Medical Necessity Argumentation | Establishing medical necessity in chiropractic requires clinical notes that describe functional status, objective findings, and measurable progress toward treatment goals — not just a diagnosis code. This is a narrative argument, not a data entry task. | Whether the clinical notes tell a coherent story of therapeutic progress. Auditors are trained to identify notes that repeat language across visits without documenting meaningful change in patient status. |
| ICD-10 Coding Specificity Demands | Chiropractic diagnoses must be coded to the highest level of specificity available — laterality, stage, acuity, and now SDOH variables under the 2026 ICD-10 updates. Generic or unspecified codes are a common audit trigger because they suggest documentation did not support a more precise classification. | Whether the diagnosis codes selected are supported by the clinical findings documented in the visit notes. Unspecified codes where specific codes were available are treated as documentation gaps. |
| Generalist Billing Logic Applied to Specialty Rules | Billing systems and billers trained on general medical coding do not have the chiropractic-specific rule set embedded in their review process. They apply standard logic to a specialty with non-standard requirements — and the gaps that result are predictable and consistent. | Whether the billing patterns reflect specialty-level knowledge or general medical logic. Auditors familiar with chiropractic documentation standards recognize when claims are being handled by someone who does not understand the specialty's unique coverage criteria. |
Why Auto-Coders Were Never Built for Chiropractic Specificity
The audit exposure isn't a mystery. It's an engineering mismatch — and it was baked in from the start.
EHR auto-coders were built to move claims. They take clinical inputs, match them against a rule set, apply codes, and submit.
That workflow is fast. It's consistent. And it's completely disconnected from the clinical judgment that determines whether a chiropractic claim survives scrutiny.
Speed and defensibility are not the same capability. Most practices only discover that gap when an audit notice arrives.
This isn't a knock on automation. Automation does exactly what it was designed to do.
But EHR billing software limits are engineered into the platform — and chiropractic is a specialty where those limits land in exactly the wrong places.
The Volume-First Engineering Problem
Auto-coders are throughput tools. Their architecture is optimized for clean claim volume — the kind where diagnosis codes map neatly to procedure codes and no modifier requires a clinical argument to justify it.
That model works in high-volume, low-complexity environments.
Chiropractic is not that environment.
NIH research on billing complexity makes this explicit: administrative and billing processes that require clinical necessity arguments can't be fully automated. The nuance required for complex appeals and documentation defense sits outside what rule-based systems can replicate.
That's not a criticism of automation. It's a precise description of what automation was designed to do — and what it was not.
Volume-first engineering deprioritizes the hard claims. Clean submissions move fast.
But the moment a claim requires a documentation review, a modifier defense, or a clinical necessity argument — the system has no pathway. The claim stalls. It ages. It dies.
And the practice never understands why.
Where Auto-Coders Break Down: AT Modifier and Maintenance vs. Active Care
The AT modifier is where auto-coders expose chiropractic practices most directly.
CMS regulations require it to differentiate acute therapeutic spinal manipulation from non-covered maintenance care. An algorithm can apply the modifier.
It cannot assess whether the clinical notes behind it establish that the care was actively therapeutic — which is the only question auditors are actually asking.
Applying a modifier and defending it are not the same thing.
A claim with the AT modifier appended but unsupported documentation is not a compliant claim. It is a liability. The modifier signals to Medicare that active therapeutic treatment occurred. The notes have to prove it.
No auto-coder reviews clinical notes against that standard.
The National Institutes of Health has confirmed it: clinical documentation quality in alternative medicine improves when human review protocols replace automated templates.
That's not a theoretical finding. A human reviewer reads the note in context. They check whether it actually substantiates the modifier being claimed. They catch the gap before the claim goes out.
Not after an auditor finds it.
Why Most Practices Don't Know Their Auto-Coder Is Failing Them
Here's what makes this particularly damaging: auto-coders don't fail loudly. They keep submitting.
Claims go out. Some get paid. The dashboard looks fine. Nothing in the system flags that the documentation behind those claims wouldn't survive a payer review.
Because the system was never designed to make that assessment.
Think of it like a smoke detector that only goes off when you press the test button. The auto-coder fires the submission. It does not tell you whether the documentation behind that claim would survive a payer review. It does not tell you whether maintenance care is being billed as active care. It does not tell you what an auditor will find when they pull the notes.
It just keeps sending claims. And the practice keeps assuming that silence means success.
By the time the exposure surfaces, the pattern is already established. Months of claims. Months of documentation gaps. All of it sitting in the record, waiting for review.
That is not a recoverable position.
It is an entirely preventable one — and prevention requires someone trained to read chiropractic notes against Medicare standards, not just to process them.
| Coding Scenario | Auto-Coder Behavior | Human Review Behavior | Audit Outcome |
|---|---|---|---|
| AT modifier application on Medicare spinal manipulation claim | Appends AT modifier automatically based on procedure code match — no review of underlying clinical notes | Reviews clinical notes to confirm documentation establishes active therapeutic care before modifier is applied | Human-reviewed claims carry defensible documentation; auto-coded claims risk denial or repayment demand if notes don't substantiate the modifier |
| Active care vs. maintenance care distinction | Cannot distinguish between the two — applies codes based on procedure input, not clinical intent documented in the note | Reads the note in context to determine whether the documented care meets Medicare's definition of active therapeutic treatment | Claims coded without this distinction are audit liabilities; human review prevents the gap from reaching the payer |
| Clinical note that incompletely documents medical necessity | Submits the claim as coded — flags nothing, moves to next claim in the queue | Identifies the documentation gap before submission and flags it for provider correction or addendum | Auto-submitted claims with weak necessity documentation create a pattern auditors identify across claim sets; human-flagged gaps are corrected before they compound |
| Transition from active care to maintenance care mid-treatment episode | Continues applying the same codes and modifiers unless the input data changes — no clinical context monitoring | Tracks the treatment arc, identifies when documentation signals a shift in care status, and adjusts coding or escalates for provider review | Billing maintenance care as active therapeutic care is one of the most common OIG error patterns; auto-coders have no mechanism to catch it mid-episode |
| Payer audit request or Additional Documentation Request (ADR) | Has no audit-response function — submission is the only workflow it supports | Reviews the claim history, assembles supporting documentation, and constructs the clinical necessity argument for the appeal | Auto-coders cannot respond to audits; a practice without human billing support faces the audit with only the documentation the algorithm produced |
| ICD-10 code specificity for chiropractic diagnosis | Matches diagnosis codes to procedure codes based on rule-set logic — selects the closest available code, not necessarily the most defensible one | Selects the most clinically accurate and audit-defensible ICD-10 code based on the documented presentation and chiropractic-specific coding standards | Imprecise diagnosis coding weakens the medical necessity argument; precise coding gives the claim structural integrity when a payer reviews it |
What the 2026 ICD-10 SDOH and Medicare Updates Actually Require

The 2026 regulatory cycle isn't a refinement. It's a structural expansion of what auditors expect to find in the clinical record — and chiropractic is directly in the crosshairs.
Two changes are landing at the same time. Updated Medicare AT modifier enforcement standards. Expanded ICD-10-CM Social Determinants of Health code blocks. Neither operates in isolation — and in 2026, that combination demands a level of clinical specificity no auto-coder is currently calibrated to meet. The gap between what the software produces and what the auditor expects is exactly where claims fall apart.
The auto-coder was already struggling before 2026. These updates add thresholds it cannot clear. That's where the human-versus-AI question stops being theoretical and starts showing up in audit notices.
ICD-10 SDOH Code Blocks and Why They Matter to Chiropractic
ICD-10-CM categories Z55 through Z65 are designated to document clinical complexities tied to socioeconomic and environmental factors. And published coding guidance makes clear that their application is expected to grow across all provider types — chiropractic included. These aren't edge-case codes reserved for primary care. They are becoming a standard documentation expectation, and practices that aren't using them are leaving clinical context out of the record.
For chiropractic, the relevance is concrete. A patient's housing instability, food insecurity, or occupational environment can materially affect both the clinical presentation and the documented rationale for active therapeutic care. When those factors are present and undocumented, the clinical notes look incomplete — not because the care was inadequate, but because the full picture wasn't captured. And an incomplete picture is exactly what a reviewer flags.
An auto-coder doesn't read the patient file for context. It maps inputs to outputs. The Z-code blocks require a clinical reader — someone who recognizes that a socioeconomic factor is present, understands its relevance to the chiropractic diagnosis, and captures it correctly. That's a clinical judgment call. No template was built to make it, and no rule-matching engine is going to start making it now.
What These Updates Mean for Active Care Documentation Standards
The AT modifier requirement hasn't changed in intent. It has always required documentation that establishes acute therapeutic spinal manipulation as distinct from non-covered maintenance care. What's changing in 2026 is the enforcement standard — specifically, how clearly that distinction must be established in the clinical record, and what reviewers will actually accept as proof. The bar isn't new. It's just higher.
Clinical notes need to actively demonstrate active care — not just assert it. Progress notes, functional outcome measures, and visit-by-visit documentation of clinical improvement are what build a defensible record. Notes that describe treatment without establishing therapeutic progress don't satisfy the standard. The code and the modifier don't fix what the underlying notes fail to prove.
Here's where the exposure compounds. An auto-coder applies the AT modifier based on the inputs it receives. It does not assess whether the underlying notes actually substantiate the modifier's clinical claim. When the 2026 enforcement standard tightens around that substantiation requirement, practices relying on auto-coders are submitting modifiers they cannot defend — and the system never flags it. That's the full scope of the auto-coder audit risk.
Who Is Not Ready for These Changes — and Who Is at Risk
The practices most exposed to the 2026 updates share a specific profile. They're billing through their EHR's built-in coding tools. They haven't done a clinical documentation review in the past twelve months. And they're treating the AT modifier as a submission checkbox rather than a clinical argument. That combination doesn't create a gap — it creates a target.
Automated billing integrations face scrutiny beyond claim accuracy. This published analysis documents how HHS enforcement actions actively penalize improper automated integration pathways that expose health datasets to unvetted scripts — a HIPAA compliance exposure that sits entirely separate from the coding problem. Practices that haven't verified their EHR's data handling workflows aren't carrying one type of exposure. They're carrying two simultaneously. Fixing the coding doesn't fix the data handling. These are not the same problem.
The practices that are ready have one thing in common: a billing partner who reads clinical notes against modifier requirements before the claim goes out — not after an auditor requests the records. The 2026 updates don't create new vulnerability for those practices. They widen the gap between the practices that have addressed their documentation standards and the ones that haven't. That gap is now visible to the same people who issue audit notices. To defend your practice against the 2026 ICD-10 SDOH updates, the documentation review has to happen before the update cycle does — not during it.
| Regulatory Update | Documentation Requirement Added | Auto-Coder Capable? | Human Review Required? |
|---|---|---|---|
| AT Modifier Enforcement Tightening | Clinical notes must actively demonstrate acute therapeutic progress — not merely assert it — through visit-by-visit functional outcome documentation | No — applies modifier based on input mapping; cannot assess whether underlying notes substantiate the clinical claim | Yes — reviewer must read notes against Medicare's active care standard before submission, not after audit request |
| ICD-10-CM SDOH Z-Code Expansion (Z55–Z65) | Socioeconomic and environmental factors affecting clinical presentation must be identified, interpreted for chiropractic relevance, and coded to the correct Z-code block | No — maps diagnosis inputs to code outputs; cannot recognize contextual patient factors or assess their relevance to the chiropractic diagnosis | Yes — clinical reader required to identify SDOH factors present in the case, understand their relationship to the diagnosis, and select the correct Z-code |
| Active vs. Maintenance Care Distinction | Documentation must establish a clear clinical boundary between active therapeutic care and non-covered maintenance care on a per-visit basis | No — cannot evaluate whether progress notes distinguish therapeutic care from maintenance care; applies codes without reading clinical context | Yes — human reviewer must confirm that each visit's notes support the active care designation before the AT modifier is submitted |
| Progress and Functional Outcome Documentation | Functional outcome measures and documented clinical improvement must appear in the record as structural evidence supporting ongoing active care authorization | No — does not audit the presence or adequacy of functional outcome documentation; processes what is submitted without evaluating completeness | Yes — reviewer must verify that outcome measures are present, clinically coherent, and sufficient to withstand payer scrutiny |
| Automated Billing Integration Compliance | EHR data handling workflows and automated coding integrations must comply with regulatory privacy standards; unvetted scripts create dual exposure — documentation risk and regulatory risk simultaneously | No — the integration itself is the risk; automated pathways that expose health datasets to unvetted scripts are subject to enforcement action regardless of claim accuracy | Yes — billing partner must verify that data handling workflows meet compliance standards, not just that claims are being submitted |
| Clinical Notes Completeness Review | Full clinical picture — including complicating patient factors — must be captured in the record to prevent notes from appearing incomplete to auditors, even when care was appropriate | No — does not read patient files for contextual gaps; processes structured inputs and produces outputs without assessing whether the underlying record tells a defensible clinical story | Yes — reviewer reads the complete note in context, identifies missing documentation before submission, and ensures the record supports the codes and modifiers applied |
What Human Clinical Intelligence Does That Algorithms Cannot
The alert keeps firing. That is what it was built to do. But nobody in the practice knows if it means a structural fire or burnt toast.
Human clinical intelligence reads the situation. It tells the difference between a documentation gap that resolves after one appeal and a systemic pattern that invites a full payer audit. That distinction requires judgment, clinical context, and specialty knowledge. None of those live inside a rule-matching engine.
The capabilities that matter in a high-specificity audit environment are not submission capabilities. They are defense capabilities. Defense is a human job.
Reading the Clinical File, Not Just the Code
An algorithm reads inputs and maps them to outputs. A trained clinical reviewer reads the file — the progress notes, the functional outcome measures, the visit-by-visit narrative — and asks the question auditors are actually asking: does this documentation establish that active therapeutic care occurred, visit by visit, for a patient who clinically needed it?
That question doesn't have a rule-based answer. It has a clinical answer. The notes either tell a coherent story of active care and measurable progress — or they don't. The National Institutes of Health has published peer-reviewed research confirming that documentation quality in alternative medicine improves when human review protocols replace automated templates. Human reviewers catch contextual gaps that pattern-matching systems are structurally blind to.
Z-code documentation requires a clinical reader. Someone who recognizes that a patient's environmental or socioeconomic factors are present, understands their relevance to the chiropractic diagnosis, and captures them with the specificity the coding standard demands. An auto-coder processes what it's given. It doesn't read for context. And that gap becomes visible the moment a reviewer pulls the record — which is why practices billing through automated systems need to understand the 2026 SDOH code expansion. the 2026 SDOH code expansion
Constructing a Medical Necessity Argument Under Audit
When a payer audits a chiropractic claim, they are not asking whether the modifier was appended. They are asking whether the documentation proves it.
Constructing a medical necessity argument is not a coding task. It's a clinical reasoning task applied to a billing record. It requires someone who understands what active therapeutic care looks like in chiropractic documentation, what Medicare's evidentiary standard actually demands, and how to separate the notes that support the argument from the ones that undermine it. McKinsey's analysis on healthcare billing complexity is direct: the nuance required for complex appeals sits outside what automated systems can replicate.
An embedded billing partner reviews the clinical record before the claim goes out. They check whether the notes actually substantiate the modifier being claimed. They flag the gap while it's still correctable. That's prevention. What happens after an auditor requests the records is remediation — and remediation is slower, more expensive, and far less reliable.
This Is Not for Every Practice
This isn't a fit for every practice. It's worth being direct about that.
Practices billing primarily cash-pay, operating without real insurance complexity, or expecting a fully disengaged arrangement — this model isn't built for them. Effective embedded billing requires cooperation: EHR access, documentation turnaround, and provider availability when a clinical record needs to be strengthened before a claim goes out. Practices that won't engage in that process won't get the outcome the process produces.
But for the chiropractic practice carrying real Medicare volume, working through the 2026 documentation requirements, and running on an EHR auto-coder that has never been stress-tested against a payer audit — that is the gap Bushido Billing was built to close. Not because the automation is broken. Because defense requires a human.
| Billing Task | Algorithm Output | Human Clinical Intelligence Output |
|---|---|---|
| AT Modifier Application | Appends modifier based on code inputs received — does not assess whether underlying clinical notes substantiate the active care claim | Reviews progress notes and functional outcome measures to confirm the documentation establishes active therapeutic care before the modifier is applied |
| Z-Code SDOH Documentation | Maps available inputs to available codes — does not read the patient file for socioeconomic or environmental context | Identifies whether a patient's housing, occupational, or social factors are clinically present, understands their relevance to the chiropractic diagnosis, and captures them with coding specificity |
| Maintenance vs. Active Care Distinction | Applies the code category that matches the submitted inputs — cannot evaluate whether the visit-by-visit narrative demonstrates therapeutic progress | Reads the clinical record to determine whether documented improvement supports active care classification or whether the notes expose a maintenance care pattern |
| Medical Necessity Argument Construction | Cannot construct a clinical reasoning argument — produces a coded output, not a defense narrative | Builds a cohesive medical necessity argument from the clinical record, identifying which notes support the claim and which create vulnerability |
| Pre-Submission Documentation Review | Submits claims based on EHR data as entered — no gap-identification step before transmission | Reviews the clinical record against modifier requirements and payer standards before the claim is submitted, flagging correctable gaps while they are still correctable |
| Denial Pattern Recognition | Flags individual claim rejections — does not identify systemic documentation patterns driving recurring denials | Tracks denial patterns across claims to identify root causes in clinical documentation, coding specificity, or modifier application — and addresses them at the source |
| Payer Audit Response | Has no pathway for constructing or submitting a clinical appeal — audit response falls entirely to the practice | Prepares the clinical record for audit defense, assembles the supporting documentation, and constructs the appeal argument from specialty-level knowledge of what payers are actually evaluating |
How to Evaluate Whether Your Current Coding Is Audit-Ready
The audit doesn't start when the letter arrives. It starts the moment the claim is submitted — and at that point, the documentation record is fixed. It either supports the modifier or it doesn't. The only window to fix that is before submission.
Most chiropractic practices don't know their audit exposure until they're already inside one. The OIG repeatedly targets chiropractic claims for high billing error rates driven specifically by missing medical necessity indicators. And the pattern in those reviews is consistent: the documentation existed — it just didn't establish active therapeutic care clearly enough to satisfy the evidentiary standard. Good faith isn't a defense. Clear notes are.
Here's the thing: that gap is diagnosable before an auditor finds it. The questions below are what a clinical reviewer asks when stress-testing a billing setup against real payer scrutiny. If your current billing arrangement can't answer them clearly, you already have your answer.
Five Questions to Ask Your Current Billing Setup
First: Does someone review clinical notes against modifier requirements before the claim goes out — not after? An AT modifier appended without a prior clinical note review is an assertion. Not a defense. When the OIG pulls chiropractic records, they're asking one thing: does the documentation prove what the modifier claims? Not whether the modifier was appended. If your answer is "the EHR handles that" — the practice isn't audit-ready.
Second: Has your billing setup been stress-tested against a payer audit scenario in the past twelve months? A setup that's never been reviewed against actual audit criteria is a smoke detector that's never been tested. It fires on submission. Nobody knows whether it holds up under scrutiny.
Third: Does your EHR's automated integration pathway meet current data handling standards? HHS enforcement actions penalize improper automated integration pathways that expose health datasets to unvetted scripts. Practices running unverified EHR billing integrations carry two categories of exposure at once — documentation risk and regulatory compliance risk. Most don't know the second one exists until an enforcement action surfaces it.
Fourth: Can your visit notes demonstrate clinical improvement visit by visit — or do they describe treatment without establishing therapeutic progress? Notes that document what the provider did without establishing that the patient improved don't satisfy the Medicare active care standard. Payers are trained to find that distinction.
Fifth: Does your billing partner flag documentation gaps before submission — or do you find out about problems when a denial arrives? Denials are a lagging indicator. By the time the denial lands, the claim is already in a reactive posture. A billing setup built for audit defense finds the gap while it's still correctable — before the record is fixed in the payer's system.
If three or more of those questions don't have a clear, confident answer — the exposure is real. And it's already accumulating in your AR.
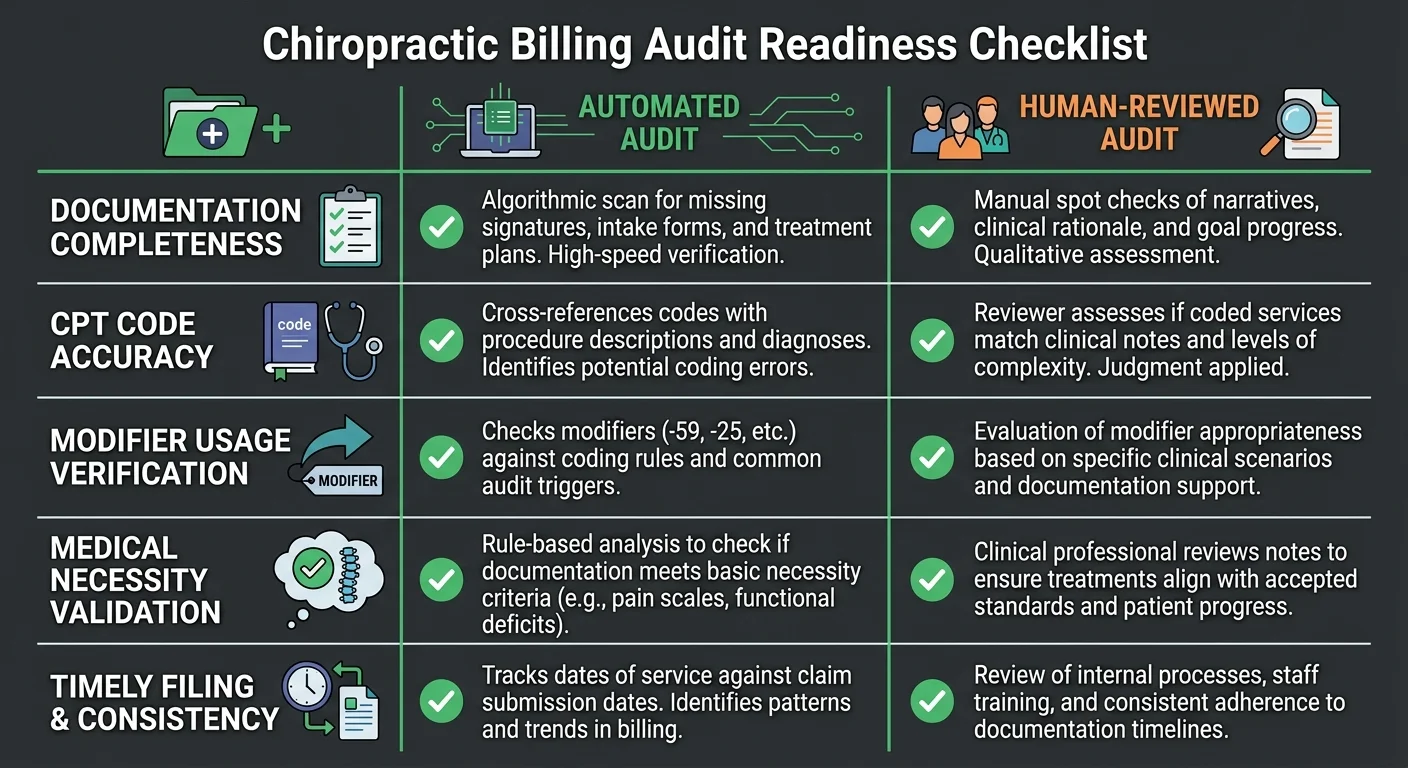
What an Audit-Ready Billing Review Actually Covers
An audit-ready billing review isn't a compliance checklist. It's a clinical documentation review conducted against the specific evidentiary standards payers use when they pull records. Those are not the same thing — and the difference is what most practices find out too late.
That review covers four layers. First is modifier substantiation — whether the AT modifier is supported by visit-by-visit documentation that establishes active therapeutic care and measurable functional progress. Second is coding specificity — whether the ICD-10 codes reflect the clinical presentation with enough precision to survive payer scrutiny, including any applicable SDOH factors that affect the diagnosis rationale. Third is integration hygiene — whether the EHR's automated data pathways meet current regulatory standards for protected health information handling. Fourth is pattern analysis — whether denial patterns across the claim history reveal a systemic documentation gap or isolated errors. For practices already concerned about EHR auto-coder audit risk, it's that fourth layer where the systemic gaps become impossible to ignore.
The smoke detector tells you a claim was submitted. An audit-ready review tells you whether the documentation behind that claim holds up when a payer asks the only question that actually matters: does this record prove that active therapeutic care occurred, visit by visit, in a patient who needed it? Submitting a claim and defending a claim are two entirely different jobs. Every practice can run that diagnostic before an auditor does it for them.
| Audit Readiness Signal | Auto-Coder Setup | Human-Embedded Billing Setup |
|---|---|---|
| Modifier review before submission | AT modifier appended automatically at claim generation — no clinical note review occurs before submission | Human reviewer reads visit notes against the AT modifier standard before the claim goes out — gaps are correctable at this stage |
| Medical necessity argument construction | System processes what the note contains — cannot identify whether the documentation tells a coherent story of active therapeutic progress | Billing partner reads the clinical record as a payer auditor would and builds the necessity argument from the documentation, not around it |
| Denial pattern identification | Denials are processed individually — systemic documentation gaps driving recurring denials are not surfaced or analyzed | Denial history is reviewed for patterns — recurring gaps are traced to their documentation source and corrected upstream |
| SDOH and ICD-10 coding specificity | Auto-coder applies codes based on structured data fields — contextual clinical factors like applicable Z-codes are not recognized or captured | Reviewer identifies clinically relevant socioeconomic or environmental factors in the record and applies ICD-10 specificity the documentation actually supports |
| EHR integration compliance | Automated data pathways operate as configured — regulatory changes to PHI handling standards are not monitored or flagged | Integration hygiene is reviewed against current regulatory standards — exposure from unvetted automated pathways is identified before an enforcement action surfaces it |
| Audit scenario stress-testing | Billing setup has never been reviewed against actual payer audit criteria — performance under scrutiny is unknown until an audit occurs | Documentation is periodically stress-tested against the evidentiary standard payers apply — audit readiness is confirmed, not assumed |
| Visit-by-visit progress documentation | Notes are submitted as entered — whether they establish measurable functional progress visit by visit is not assessed before claim generation | Reviewer evaluates whether each visit's notes satisfy the active care standard independently — not just whether treatment was documented, but whether improvement was established |
Frequently Asked Questions
Strategy is one thing. What practitioners want to know is simpler: will their current setup hold up when a payer pulls their records?
These answers get into that directly.
Six questions. What the technology does. Where it breaks. What that costs. And what a human-embedded model actually looks like when the audit clock is running.
How do automated EHR coding tools increase chiropractic audit risk?
Auto-coders submit. They don't verify.
The OIG has flagged chiropractic claims as a high-error category for years. The pattern driving those errors isn't random billing mistakes — it's a predictable output of systems that append modifiers without first confirming the clinical notes behind those modifiers can actually hold up under review.
Here's how it plays out: the AT modifier fires on submission. The documentation behind it may not satisfy the evidentiary standard an auditor is applying. That gap — between what the modifier asserts and what the notes prove — is where audits find their footing. The auto-coder never flags it. The practice never sees it coming.
Why can't AI coding tools distinguish active therapeutic care from maintenance care?
The distinction isn't in the code. It's in the notes.
CMS requires the AT modifier to separate acute therapeutic spinal manipulation from non-covered maintenance care. Figuring out which category a visit falls into means reading the clinical record — specifically, whether the documentation shows measurable functional progress and treatment toward a defined therapeutic goal. That's a clinical assessment. Not a syntax check.
An algorithm reads code fields. It doesn't read visit notes for evidentiary quality. McKinsey's analysis on healthcare billing complexity confirms it directly: complex claims that rely on clinical necessity arguments sit outside what automated systems can replicate. The active-versus-maintenance distinction is exactly that kind of argument. It requires someone who understands what active care looks like in chiropractic documentation. No EHR auto-coder does that review.
How do the 2026 ICD-10 SDOH updates affect chiropractic claim audits?
They raise the specificity bar in a place auto-coders were already falling short.
CDC designates ICD-10-CM categories Z55 through Z65 to document Social Determinants of Health — clinical variables tied to socioeconomic and environmental factors that affect both how a patient presents and why active therapeutic care is warranted. For chiropractic claims under the 2026 framework, that means diagnosis codes now need to reflect the full clinical picture, including SDOH factors that explain the patient's presentation, what the treatment plan is actually addressing, and how progress is being measured.
An auto-coder selects codes from the EHR data it can access. It doesn't assess whether those codes reflect the clinical presentation with the precision the 2026 updates demand. That requires a human reviewer reading the patient file for contextual factors — not a system mapping inputs to outputs and moving to the next claim.
What does it actually cost a practice when an auto-coder fails during a Medicare audit?
The visible cost is denied and recouped revenue. That's the number practices see.
But the deeper cost is the remediation posture. Once an audit is open, the clinical record is fixed. The documentation either supports the claim or it doesn't. Remediation means working backward through records that can't be corrected — building the strongest possible argument from whatever the notes contain — while absorbing an appeal process that costs far more than prevention would have.
McKinsey's analysis on healthcare billing complexity is direct: the nuance required for complex appeals and documentation defense sits outside what automated systems can replicate. A practice that relied on an auto-coder for submission and had no embedded clinical reviewer finds out, inside an audit, that submission speed and documentation defense are not the same capability. They're not interchangeable once the letter arrives.
How does an embedded human billing partner defend coding specificity that software cannot?
By reviewing the clinical record before the claim goes out.
An embedded human billing partner reads the visit notes against the modifier requirements. They assess whether the documentation establishes active therapeutic care clearly enough to satisfy the evidentiary standard an auditor would apply. They flag the gap while it's still correctable — before the record is locked in the payer's system. That's prevention. What happens after an auditor requests the records is remediation. Those are not the same conversation.
There's a second layer most practices miss entirely. HHS enforcement actions actively penalize improper automated integration pathways that expose health datasets to unvetted scripts. An embedded clinical reviewer who understands EHR integration hygiene catches that exposure category too — before it surfaces as a separate enforcement action. One review. Two categories of risk. Addressed before either one becomes a crisis.
Is a DC-founded billing company actually better positioned to handle these audits?
Yes. And the reason is specific, not promotional.
The OIG's chiropractic audit focus is built on a clinical understanding of what active therapeutic care looks like in documentation. Defending against that scrutiny requires someone who understands the clinical standard from the inside — what the notes need to show, how chiropractic progress is measured and documented, and where evidentiary gaps hide in a typical practice's records.
Bushido Billing was co-founded by a chiropractor. That's not a marketing angle — it's a prerequisite for the kind of clinical documentation review that closes the gap between what an auto-coder submits and what a payer auditor actually demands. Peer authority here means the billing partner has run a chiropractic practice and knows exactly what an audit looks like from the provider's side of the table.
Submitting a claim and defending a claim are two entirely different jobs. One requires that kind of knowledge. The other just requires software.
The Verdict: Detection Is Not Defense
The auto-coder does its job. Claims go out clean, fast, and on time.
But the moment a payer pulls that claim and asks whether the documentation proves what the modifier asserts — the auto-coder has nothing to say.
That question belongs to a different system entirely.
Submitting a claim and defending a claim are two different jobs. Not versions of the same job.
Submission is a transaction. Defense is a clinical argument — built from progress notes, functional outcome measures, and visit-by-visit documentation that establishes active therapeutic care in language auditors accept as proof.
No algorithm builds that argument. Not because the technology is immature. Because the work requires clinical reasoning, not pattern recognition. Those aren't the same capability. Submission speed doesn't close that gap — it just gets you to the audit faster.
Bushido Billing was built for this specific problem — in this specific specialty.
The 2026 Medicare and ICD-10 updates don't change the fundamental question auditors have always asked. They raise the evidentiary bar for answering it. And for any chiropractic practice running real Medicare volume through an auto-coder, the documentation record being built right now is either defensible or it isn't.
Detection is not defense. The practices that understand that difference before the audit letter arrives are the ones that don't need to explain it afterward.
The 2026 updates don't create new risk. They expose the risk that's already sitting in your claims. If your billing setup can submit but can't defend, that gap is now visible to the people issuing audit notices. Book a Call to see where Bushido Billing finds it before a payer does.
Book a Call to see where your coding stands before a payer does

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet