

How to Document Maintenance vs. Active Care to Withstand a 2026 Insurance Audit
Documenting active care versus maintenance care for a 2026 insurance audit requires a clear, visit-by-visit clinical record showing measurable patient improvement tied to a specific treatment plan with objective functional benchmarks. The distinction is not administrative. It is the legal basis for every Medicare chiropractic claim.
Active care documentation must demonstrate that spinal manipulation services are corrective and medically necessary. Medicare requires the AT modifier on Part B claims to indicate that the service constitutes active, corrective treatment rather than maintenance therapy. Medicare excludes maintenance therapy from coverage entirely. Without documentation that supports that modifier at every single visit, the claim is indefensible the moment an auditor opens the file.
Maintenance care operates under a different clinical profile. It focuses on preventing recurrence and optimizing function. It uses structured, scheduled visits regardless of symptom status. That profile does not satisfy the coverage criteria for active, restorative episodes.
Local Coverage Determinations require active care documentation to show patient improvement within a reasonable, predictable timeframe. Treatment plans must target measurable functional limits, supported by objective metrics such as pain scales and baseline functional questionnaires. National chiropractic clinical documentation frameworks recommend functional reassessments every two to four weeks of active treatment to maintain that evidentiary chain.
Office of Inspector General audits of chiropractic claims consistently find error rates exceeding 50% for targeted codes. Clinical progression notes repeatedly fail to support the active care designations submitted on those same claims.
The documentation standard for 2026 is not more complex than prior years. The enforcement pressure is. Every reassessment, every updated treatment plan, every clinical note functions as either a defense or a liability. The practices that survive audits intact are the ones that built the record before the auditor ever asked for it.
Last Updated: June 22, 2026
- • Why the Active vs. Maintenance Line Is the First Thing Auditors Look For
- • Why Most Billing Systems Miss the AT Modifier Flag Before Submission
- • The Clinical Documentation Standard That Separates Active from Maintenance Care
- • What Happens When a Practice Cannot Produce the Documentation in an Audit
-
• Frequently Asked Questions
- • What is the primary documentation difference between active care and maintenance care?
- • How do auditors evaluate the AT modifier on 2026 chiropractic claims?
- • What objective clinical metrics must be documented to prove active corrective care?
- • Does a plateau in patient progress automatically classify subsequent visits as maintenance care?
- • How does a performance-aligned billing partner help prevent active care documentation audits?
- • Can a chiropractic practice bill active care and maintenance care for the same patient in the same year?
- • Documentation Is the Practice's Defense — Build It That Way
Why the Active vs. Maintenance Line Is the First Thing Auditors Look For
Auditors don't open your billing records first. They open your clinical story — and the first question they're answering is whether your treatment was active care or maintenance care.
This isn't a technicality buried in a billing manual. It's the foundational coverage question — the one that determines whether Medicare owes the practice anything at all.
Get it wrong in the documentation, or fail to document it clearly, and every claim tied to that patient becomes a recoupment target.
OIG audit findings on chiropractic claims put the error rate for targeted codes above 50%. The consistent driver isn't upcoding or modifier fraud — it's clinical progression notes that don't support the active care designation on the claim.
A paper trail is either a shield or a liability. Auditors know which one they're looking at before they finish the first chart.
The Coverage Rule That Creates the Risk
Medicare covers spinal manipulation only when it constitutes active, corrective treatment. That's not an interpretation. That's the rule.
The AT modifier on Medicare Part B claims is what signals active, corrective treatment to the payer. And Medicare excludes maintenance therapy from Part B coverage entirely — no exceptions, no gray area.
So here's what that means in practice: every appointment without documentation that earns the AT modifier is a claim billed without a legal foundation.
NIH research on chiropractic care classification is precise about this — the clinical distinction between active and maintenance treatment is defined by the presence or absence of measurable corrective progress. Not patient preference. Not visit frequency. Not provider intent.
The coverage rule creates the risk. The documentation either neutralizes it or compounds it. There's no middle ground — and in 2026, enforcement pressure makes that binary more consequential than it's been in years. how coverage rules intersect
Why Volume-First Billing Platforms Miss This Distinction Every Time
Volume-first billing platforms are built for one thing: getting claims out the door fast. They're optimized for submission speed. Not for the documentation integrity that has to hold up when a post-payment audit arrives.
Catching the active vs. maintenance distinction requires a human to evaluate the clinical record against the AT modifier criteria before the claim goes out.
Not after a payer flags it. Before.
Automated claims-pushing has no mechanism for that review. The system doesn't read the SOAP note. It reads the code.
That's how a practice ends up with a clean claim submission rate and a six-figure recoupment demand at the same time.
Submission accuracy and documentation sufficiency are not the same standard. One measures whether the claim was formatted correctly. The other measures whether the underlying visit can be defended when an auditor pulls the chart.
The full-service insurance billing model Bushido Billing operates on treats every chiropractic claim as a document that must be defensible — not just transmittable.
That gap between submission and defense is where most practices are exposed. And it's exactly where most audits find their opening.
| Category | Medicare Coverage Status | AT Modifier Required | Clinical Basis |
|---|---|---|---|
| Active Corrective Care | Covered under Medicare Part B when properly documented | Required — signals active, corrective treatment to the payer | Measurable functional improvement toward a defined clinical endpoint within a predictable timeframe |
| Maintenance Care | Excluded from Medicare Part B coverage | Not applicable — maintenance therapy does not qualify for the AT modifier | Prevention of recurrence and optimization of function; structured visits regardless of symptom status or measurable progress |
| Undocumented or Ambiguous Care | Effectively excluded — payer defaults to non-coverage without clear clinical justification | Undefended — AT modifier submitted without supporting documentation becomes the audit target | No distinguishable clinical basis; the record does not tell the corrective-versus-maintenance story auditors require |
Why Most Billing Systems Miss the AT Modifier Flag Before Submission
Knowing the difference between active care and maintenance care doesn't protect your practice. What happens inside the billing workflow before that claim leaves your system — that's where the exposure is.
Most billing systems aren't evaluating clinical intent. They're validating code format. The AT modifier gets appended from a submission template — not because anyone reviewed whether the visit documentation actually supports active, corrective treatment.
That's not a technical limitation. It's a design choice. Volume-first billing platforms are built for throughput, not for audit defense. The modifier goes on the claim. Whether the chart earns it is a different question — and most automated workflows never ask it.
What Automated Claim Submission Actually Checks — and What It Skips
Here's what automated claim submission actually does: it checks that required fields are populated and codes are formatted correctly for the payer. That's it. It doesn't read the SOAP note. It doesn't verify that the clinical narrative supports the active care designation you're staking the AT modifier on.
What gets skipped is the only layer that matters on audit: clinical progression evidence. An auditor pulls the chart and asks one question — does each visit show measurable corrective progress tied to a defined treatment plan? EHR platforms marketed as billing solutions are submission tools. They can't answer that question. Only a human who understands the coverage standard can.
The same gap shows up anywhere coding requires contextual clinical judgment rather than format compliance. Automated workflows apply rules. They don't apply judgment. And on a Medicare chiropractic audit, judgment is the only thing that holds — including on decisions tied to the G2211 add-on code.
Who This Billing Model Fails First
This model fails Medicare-heavy practices first, and it fails them visibly. Error rates for targeted chiropractic codes exceed 50% — and the driver isn't wrong code selection. It's clinical progression notes that don't support the active care designations on the claims. The code was right. The chart didn't back it up.
It also fails practices at the transition point — providers moving patients from acute active care toward the visit where maintenance care becomes appropriate. That clinical handoff demands a deliberate, documented shift in narrative. Automated claims-pushing has no mechanism to flag that the chart needs to change before the code does. So the code changes. The chart doesn't. And the audit finds the gap.
A paper trail is either a shield or a liability. The billing model determines which one gets built. A system optimized for submission speed produces claims that look clean until an auditor reads the chart. An embedded, human-driven billing partnership catches the documentation gap before the claim goes out — because that's where the defense is won or lost.
| Billing Approach | AT Modifier Verification | Documentation Review Pre-Submission | Audit Exposure Level |
|---|---|---|---|
| Volume-first automated billing platform | AT modifier appended via submission template — no clinical review performed | None — system validates code format, not clinical narrative | High — claims look clean on submission; chart fails under auditor review |
| EHR-integrated billing module | AT modifier populated from encounter data fields — no cross-check against active care criteria | None — documentation sufficiency is assumed, not verified | High — EHR confirms the visit occurred; it cannot confirm the visit qualifies as active, corrective treatment |
| Embedded, human-driven billing partnership | AT modifier verified against clinical progression notes before submission — documentation must earn the modifier | Pre-submission review confirms SOAP note supports active care designation and measurable corrective progress | Low — the defense is built into the claim before it leaves the practice, not reconstructed after an auditor requests the chart |
The Clinical Documentation Standard That Separates Active from Maintenance Care
So what does defensible active care documentation actually look like, visit by visit?
Not abstract. Not general. Concrete and measurable — every single appointment.
It starts with the treatment plan. Not a general narrative about the patient's condition — a plan that targets measurable functional limits and defines what improvement looks like in observable terms.
Local Coverage Determinations are direct on this: active care must demonstrate patient improvement within a reasonable, predictable timeframe. A plan without measurable benchmarks is a plan an auditor will dismantle in minutes.
Goals that can't be measured can't be defended.
Maintenance care tells a different story. Structured, scheduled visits that occur regardless of symptom status — that clinical picture has a name, and auditors are trained to recognize it on sight.
The documentation standard doesn't demand perfection. It demands evidence that the treatment was going somewhere — that each visit moved the patient measurably closer to a defined clinical goal.
When the chart can't show that trajectory, it shows a maintenance profile instead. And a maintenance profile is not a covered service under Medicare Part B.
The Objective Metrics That Make Active Care Defensible
Objective metrics aren't a documentation bonus. They're the evidentiary floor that makes the AT modifier defensible when published coverage data is what an auditor is reading against your chart.
No metrics. No defense.
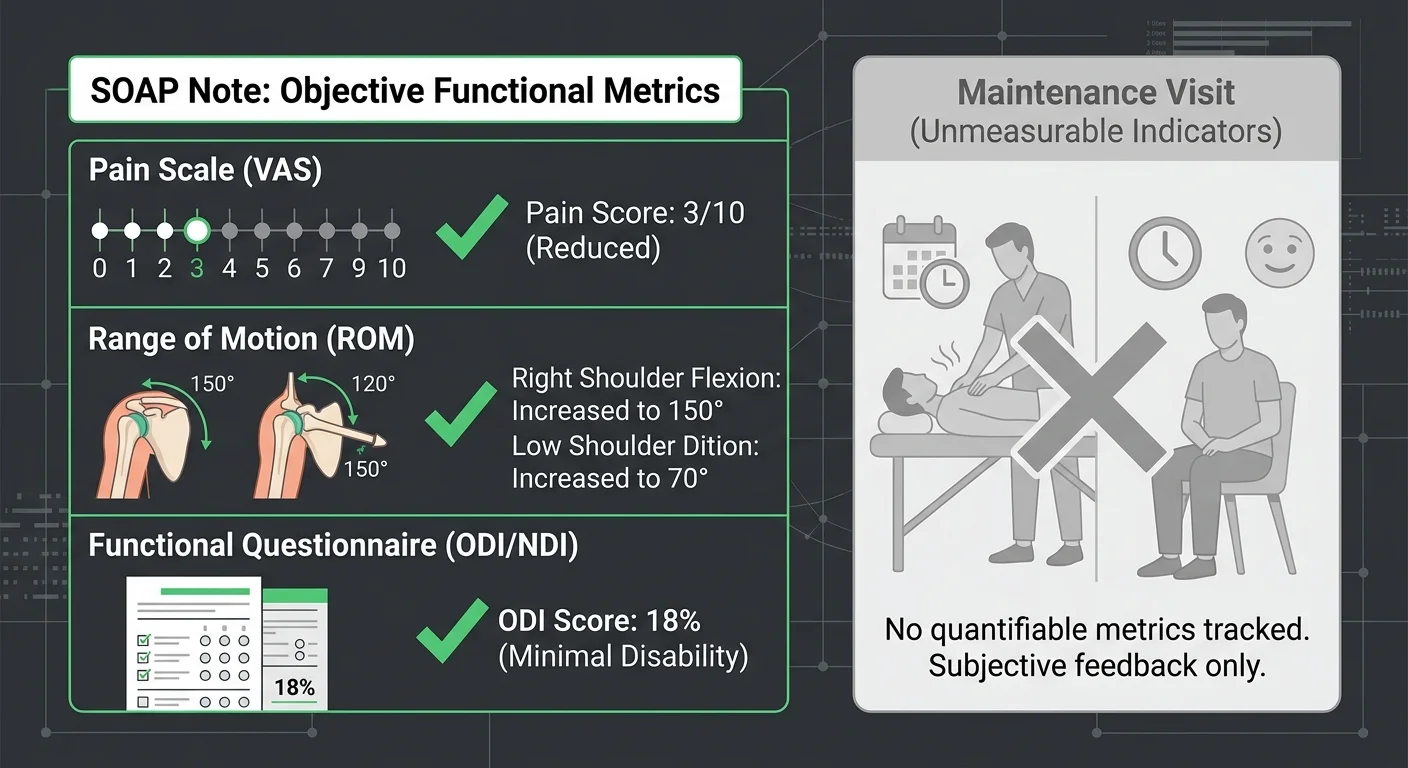
Pain scales and baseline functional questionnaires are the minimum threshold. What auditors look for beyond that is a trajectory.
Visit-over-visit documentation showing the patient's functional status moving in a measurable direction — tied directly to the stated treatment goals. That's the standard.
Static documentation is the fastest path to a maintenance care reclassification. When the clinical narrative reads the same from one visit to the next, the chart isn't describing active treatment. It's describing a routine.
Objective evidence is what converts a clinical encounter into a covered service. But objective metrics alone don't hold if the diagnosis code is doing no work.
Vague or unspecified codes strip the specificity that makes clinical narrative documentation coherent. The code and the chart have to tell the same story — same patient, same condition, same measurable trajectory. When they don't align, the modifier has no anchor and the claim has no foundation.
That alignment failure is one of the most reliable audit triggers in chiropractic billing. It shows up consistently — documented in detail — in audit triggers for unspecified codes.
The Re-Evaluation Cadence CMS Expects to See
Federal Medicare regulations governing active care billing don't leave re-evaluation frequency to clinical judgment. National chiropractic documentation frameworks put the number at every two to four weeks of active treatment.
That cadence isn't a recommendation. It's the rhythm CMS looks for in the chart when it's deciding whether the active care designation holds.
A chart without that rhythm tells one story: the practice was managing a schedule, not tracking a patient.
Each reassessment has to do two things — and both matter.
Confirm the patient is responding. Then update the treatment plan to reflect where the patient actually is now, not where they were at intake.
A reassessment that restates the original plan tells an auditor the practice wasn't paying attention. That's autopilot. And autopilot is the clinical signature of maintenance care — the designation that pulls Medicare coverage off the visit entirely.
The re-evaluation cadence is where most audit vulnerabilities are created.
Not by providers who skip reassessments. By providers whose reassessments don't show functional change — the one thing that separates active treatment from scheduled wellness management.
The paper trail has to show movement. Or it shows nothing worth defending.
If You Cannot Prove Progression, You Cannot Bill Active Care
Progression isn't implied by how often a patient shows up. It isn't assumed from the diagnosis code.
It's documented — or it doesn't exist. And if it doesn't exist in the chart, the AT modifier has no clinical foundation to stand on.
Here's the failure mode that catches providers off guard: clinical correctness is not audit protection.
A provider can be exactly right — the patient was receiving active, corrective treatment — and still lose an audit because the chart reflects the maintenance care profile. Fixed visit schedules. Absent functional metrics. No updated treatment goals.
Auditors don't evaluate the clinical reality. They evaluate the documented clinical reality. Those are not always the same thing.
If the chart cannot prove progression, the claim cannot prove active care. National documentation frameworks draw precise distinctions between therapeutic encounters and general wellness visits — and auditors apply those same distinctions when they're deciding whether the billing reflects real clinical intent.
The practices that walk out of 2026 audits intact didn't build their paper trail after the auditor asked for it. They built it visit by visit, treating every SOAP note as the legal document it actually is.
A paper trail is either a shield or a liability. The documentation standard is what determines which one you hand the auditor.
| Documentation Element | Active Care Requirement | Maintenance Care Profile | Audit Risk If Missing |
|---|---|---|---|
| Treatment Plan | Targets measurable functional limits with defined, time-bound goals and a projected endpoint for corrective care | Scheduled visits structured around prevention of recurrence, with no defined corrective endpoint or functional target | Auditor reclassifies all visits under plan as maintenance — AT modifier loses support across the entire claim series |
| Objective Metrics | Pain scales, baseline functional questionnaires, and outcome tools recorded at intake and updated at each reassessment to show directional progress | Symptom status tracked informally or not at all — visit notes describe patient condition without quantified comparison to a prior baseline | No evidentiary foundation to defend the active care designation; clinical narrative cannot demonstrate the improvement trajectory required under coverage standards |
| Functional Reassessments | Conducted on a regular cycle throughout the active treatment course, each confirming treatment response and updating the plan to reflect the current clinical picture | Absent or perfunctory — original plan restated without update, signaling to reviewers that no new clinical evaluation occurred | Chart reads as autopilot management rather than active correction; strongest single indicator of maintenance care misclassification on audit |
| SOAP Note Narrative | Visit-over-visit documentation reflects measurable change in patient function tied directly to the stated treatment goals and current plan | Clinical narrative is static — language, findings, and assessment repeat from visit to visit with no documented progression | Static notes are the fastest path to maintenance care reclassification; auditors are trained to flag identical or near-identical narrative across a claim series |
| AT Modifier Justification | Modifier is supported by a documented clinical rationale present in each visit note — active treatment designation is earned by the chart, not appended by template | Modifier applied as a submission default without a corresponding clinical narrative that distinguishes the visit from a scheduled wellness encounter | Modifier has no clinical foundation when chart is reviewed; recoupment demand applies retroactively to every claim where the modifier cannot be independently justified |
| Diagnosis Code Specificity | Diagnosis codes reflect the specific, active condition being treated — aligned with the functional metrics and treatment goals documented in the plan | Unspecified or broadly coded diagnoses that do not anchor to a measurable clinical presentation or corrective treatment objective | Vague codes strip coherence from the entire documentation set; objective metric documentation loses meaning when the condition it measures is not specifically identified |
What Happens When a Practice Cannot Produce the Documentation in an Audit
When the documentation isn't there, the outcome isn't ambiguous.
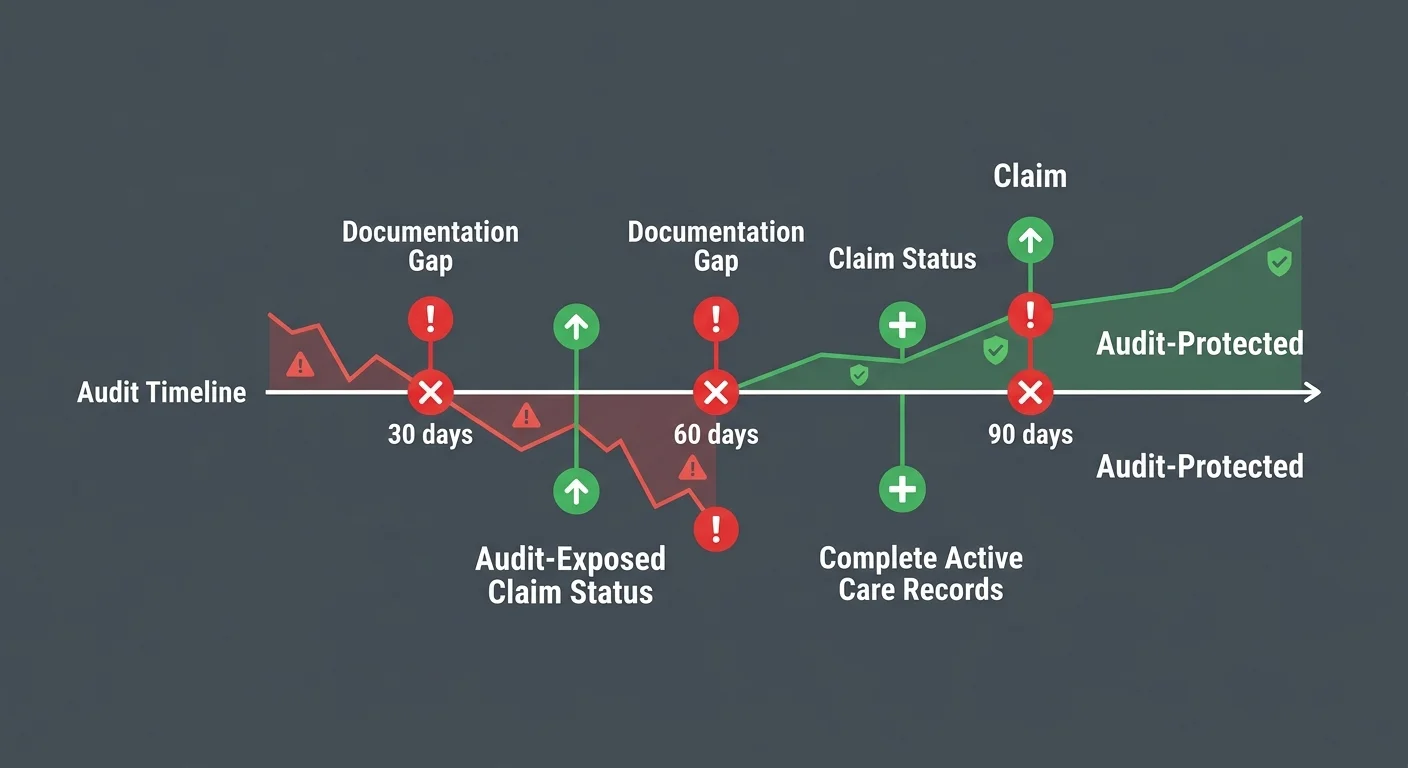
The claim gets recouped. The payment the practice already received gets taken back — and recoupment demands don't cover just the flagged visit. They cover the entire audited claim pool.
That pool can span years. Medicare audits are retrospective.
Bill active care visits over a 24-month window without solid progression documentation and you're not defending one bad claim. You're handing back every payment tied to that documentation pattern.
The absence of documentation is not a paperwork problem. It is a revenue liability that compounds with every visit billed.
And the compounding starts long before any auditor shows up.
The OIG Audit Pattern and What It Targets in Chiropractic Claims
The Office of Inspector General doesn't audit randomly. It targets patterns.
Chiropractic claims appear on its work plan year after year because the error rates for targeted chiropractic codes exceed 50%. And the driver isn't upcoding or wrong code selection. It's clinical progression notes that don't support the active care designations submitted on those same claims.
What auditors look for is a gap between what the AT modifier declares and what the chart proves.
Local Coverage Determinations are direct: active care documentation must show patient improvement within a reasonable, predictable timeframe. When the chart shows fixed-interval visits, absent functional metrics, and no updated treatment goals, the auditor has already identified the documentation profile of maintenance care. It doesn't matter what the provider intended clinically.
The chart is the record. The record is the verdict.
The OIG isn't looking for bad actors. It's looking for the documentation gap that volume-first billing produces at scale.
Practices that have never been audited aren't safe. They're simply next. The gap accumulates visit by visit — invisible until a retrospective pull makes it catastrophically visible. auto-coding workflows carry distinct audit exposure
This Is Not the Practice to Be If You Only See Billing After a Denial
Here's the practice profile that carries the highest audit exposure: the one that only looks at billing when a claim comes back denied.
Denial-first billing is reactive by design. The documentation problem — the one that fails the audit — was built visit by visit, long before any denial signal surfaced. By the time a denial arrives, the exposure already exists across every claim in the retrospective window.
Recoupment demands don't arrive with enough lead time to reconstruct a chart. The documentation either exists in real time or it doesn't exist at all.
Embedded billing partner communication built around weekly visibility means the gap between what the chart says and what the claim declares gets caught before it becomes an audit liability — not after a demand letter arrives.
A practice that waits for a denial to engage with its billing has already lost the audit before it starts.
A paper trail is either a shield or a liability. It gets built one SOAP note at a time — long before any auditor ever requests it.
| Audit Scenario | Documentation Gap | Likely Auditor Finding | Financial Consequence |
|---|---|---|---|
| Active care billed with no functional outcome metrics on file | No pain scale scores, no baseline functional questionnaires, no visit-over-visit progression data | Maintenance care reclassification — AT modifier unsupported | Full recoupment of all claims in the audited window tied to that documentation pattern |
| Static clinical narrative repeated across consecutive visits | SOAP notes read identically from one visit to the next — no updated treatment goals, no functional status change recorded | Autopilot billing profile identified — active care designation rejected | Retroactive denial across the entire claim pool sharing that documentation profile |
| Treatment plan lacks measurable functional limits | Goals described in general terms without objective benchmarks tied to the patient's stated functional deficits | Plan fails Local Coverage Determination standards for active corrective care | Claims disqualified from Medicare Part B coverage; recoupment demand issued for affected claim dates |
| Re-evaluation cadence absent or undocumented | No functional reassessments present in the chart during the active treatment period — or reassessments that simply restate the original plan without clinical update | Auditor cannot confirm treatment was responding — maintenance care profile established by default | Recoupment extended to all visits without documented progression evidence, regardless of clinical intent |
| Diagnosis code specificity misaligned with clinical narrative | Unspecified or vague diagnosis codes that conflict with or fail to support the objective metrics and treatment goals documented in the chart | AT modifier loses coherent clinical foundation — code and chart tell different stories | Compound audit exposure: coding deficiency and documentation gap assessed together, expanding the recoupment scope |
| Retrospective audit spanning a multi-year billing window | Documentation gaps are systemic across the period — not isolated to single visits — because no real-time review process caught the pattern before submission | Pattern-level finding: the practice's billing model systematically misrepresented maintenance visits as active care | Recoupment demand covers the full audited period; potential referral for further OIG review depending on error rate and claim volume |
Frequently Asked Questions
Good questions follow good audits. Here are the ones practices ask most once they start taking documentation seriously.
Each gets a direct answer. No hedging.
What is the primary documentation difference between active care and maintenance care?
Active care charts show movement. Changing functional baselines, updated treatment goals, objective metrics trending toward a defined endpoint. The story the chart tells is a patient getting better.
Maintenance care charts tell a different story. Fixed visit intervals. A clinical narrative that reads the same week to week. Scheduled visits regardless of symptom status — not incremental recovery toward a goal.
Auditors are trained to recognize both profiles on sight. And here's what they evaluate: not what the provider intended clinically, but what the chart actually documents.
If the documentation fits the maintenance profile, the AT modifier has no support. Clinical reality becomes irrelevant. The paper trail is the only reality that holds in an audit room.
How do auditors evaluate the AT modifier on 2026 chiropractic claims?
Auditors run one comparison: what the AT modifier declares versus what the chart proves.
Medicare Part B requires the AT modifier to signal active, corrective treatment. That declaration has to be earned by the clinical record — not assumed from the code. Local Coverage Determinations are explicit: the chart must show patient improvement within a reasonable, predictable timeframe.
When the chart shows fixed-interval visits, absent functional metrics, and no updated treatment goals, the modifier has no clinical foundation. The auditor doesn't need to dig. The documentation gap is visible from the first chart review.
That's the moment a claim gets reclassified. Not because the provider did anything wrong clinically. Because the chart couldn't prove they didn't.
What objective clinical metrics must be documented to prove active corrective care?
Pain scales and baseline functional questionnaires are the floor. They establish a starting point. But a starting point alone doesn't build a defense.
What auditors look for beyond that is a trajectory. Visit-over-visit documentation showing functional status moving in a measurable direction — tied directly to the stated treatment goals. That movement is what separates an active care record from a maintenance profile.
The American Chiropractic Association recommends functional reassessments every two to four weeks of active clinical treatment. Each reassessment has to do two things: confirm the patient is responding, and update the treatment plan to reflect the current clinical picture.
A reassessment that restates the original plan without reflecting functional change tells the auditor the practice is on autopilot. Static documentation is the fastest path to a maintenance care reclassification — and it's entirely avoidable.
Does a plateau in patient progress automatically classify subsequent visits as maintenance care?
A plateau doesn't automatically trigger reclassification. A plateau without a documented clinical response does.
The chart must show that the provider identified the plateau, evaluated whether the treatment approach needed to change, and made a documented clinical decision. That's the difference between managing an active case through a difficult phase and simply stopping the record.
Auditors don't flag the plateau itself. They flag the absence of anything in response to it — no updated treatment goal, no functional reassessment, no modified care plan.
A provider who responded clinically but didn't document the response has exactly the same audit exposure as a provider who didn't respond at all. The plateau is a clinical event. The AT modifier holds or falls based on what the chart shows the practice did next.
How does a performance-aligned billing partner help prevent active care documentation audits?
A performance-aligned billing partner catches the gap between what the chart says and what the claim declares before the claim transmits. Not after a demand letter arrives.
Volume-first billing platforms optimize for submission speed. They don't evaluate documentation against the AT modifier standard before the claim goes out. The OIG has documented error rates for targeted chiropractic codes exceeding 50% — and the consistent driver is clinical progression notes that don't support the active care designations on those same claims.
A billing partner operating under a performance-aligned model has a structural reason to prevent that gap. Recoupment affects collected revenue, not just submitted claims. That alignment changes what the billing review actually looks for.
Weekly visibility into the documentation standard is what makes prevention possible. The defense is built at the chart level, before the audit window opens — not reconstructed after a recoupment demand arrives.
Can a chiropractic practice bill active care and maintenance care for the same patient in the same year?
Yes — and this is one of the most misunderstood aspects of chiropractic billing.
A patient can move between active care and maintenance care within the same year. The billing can reflect both accurately, as long as the documentation supports each phase distinctly. Medicare Part B excludes maintenance therapy from coverage, so maintenance care visits can't carry the AT modifier. Active care visits require it.
The documentation must clearly delineate when one phase ended and the other began. That transition requires a functional reassessment that supports it — not just a shift in visit frequency or an encounter note that reads slightly different.
Auditors don't flag the coexistence of both care types. They flag the absence of documentation that justifies the transition point. A paper trail that handles this correctly is a demonstration of documentation discipline. One that doesn't is an open audit target.
Documentation Is the Practice's Defense — Build It That Way
Every question this article answered traces back to the same place.
Which modifier. Which metrics. Which reassessment cadence. Which gap triggers recoupment.
All of it collapses into one position: documentation discipline is a revenue protection strategy. Not a billing afterthought. Not a compliance checkbox. A defense — built visit by visit, long before any auditor in 2026 ever requests a chart.
The practices that walk away from audits intact don't win because they submit claims faster. They don't win because their EHR has a cleaner interface.
They win because someone treated every SOAP note like the legal brief it actually is.
Auditors don't evaluate what happened in the treatment room — they evaluate what's documented. A practice that can't produce clear progression evidence on demand has already lost. It doesn't matter how good the clinical work was.
That's the entire argument for an embedded billing model built around real-time documentation review — not post-denial cleanup. The defense is won at the chart, not at the appeal. Bushido Billing's position on this has never changed.
A paper trail is either a shield or a liability. The difference between those two outcomes is not clinical skill. It is not billing software. It is whether the practice built the record with intention or inherited it by accident.
The auditor is coming. The only question left is what the chart says when they get there.
If this hit close to home, the gap is still fixable — but only while the chart stays in your hands. Bushido Billing reviews your documentation against the AT modifier standard before the claim transmits. Not after a recoupment demand forces the conversation.

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet