

Why Your Current EHR's Auto-Coder May Be Increasing Your Audit Risk in 2026
EHR auto-coders increase chiropractic audit risk when their algorithmic defaults apply billing codes without confirming the clinical conditions those codes require.
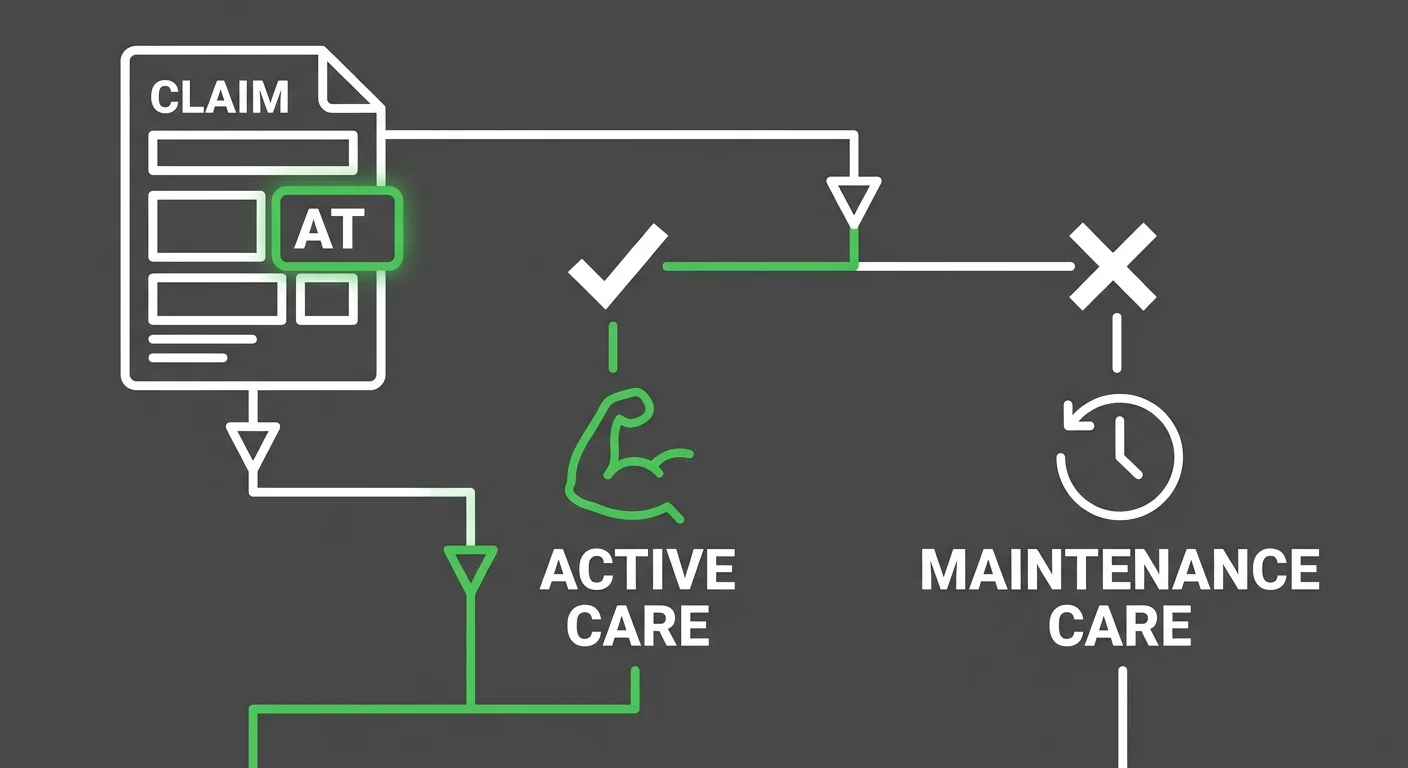
The AT modifier signals active, corrective chiropractic care to Medicare. It maps only to claims where subluxation and active treatment necessity have been manually affirmed. Auto-coding logic does not make that affirmation. It maps to what the software configuration expects — not what the clinical record actually supports on that specific date of service.
Speed is not safety.
Medicare coverage for chiropractic services is narrow by design. Manual manipulation is covered only when it corrects subluxation. Maintenance therapy is categorically excluded. When auto-coding software applies active-care modifiers across a patient's full claim history without distinguishing treatment phase, it produces the exact billing pattern that triggers retrospective recovery audits.
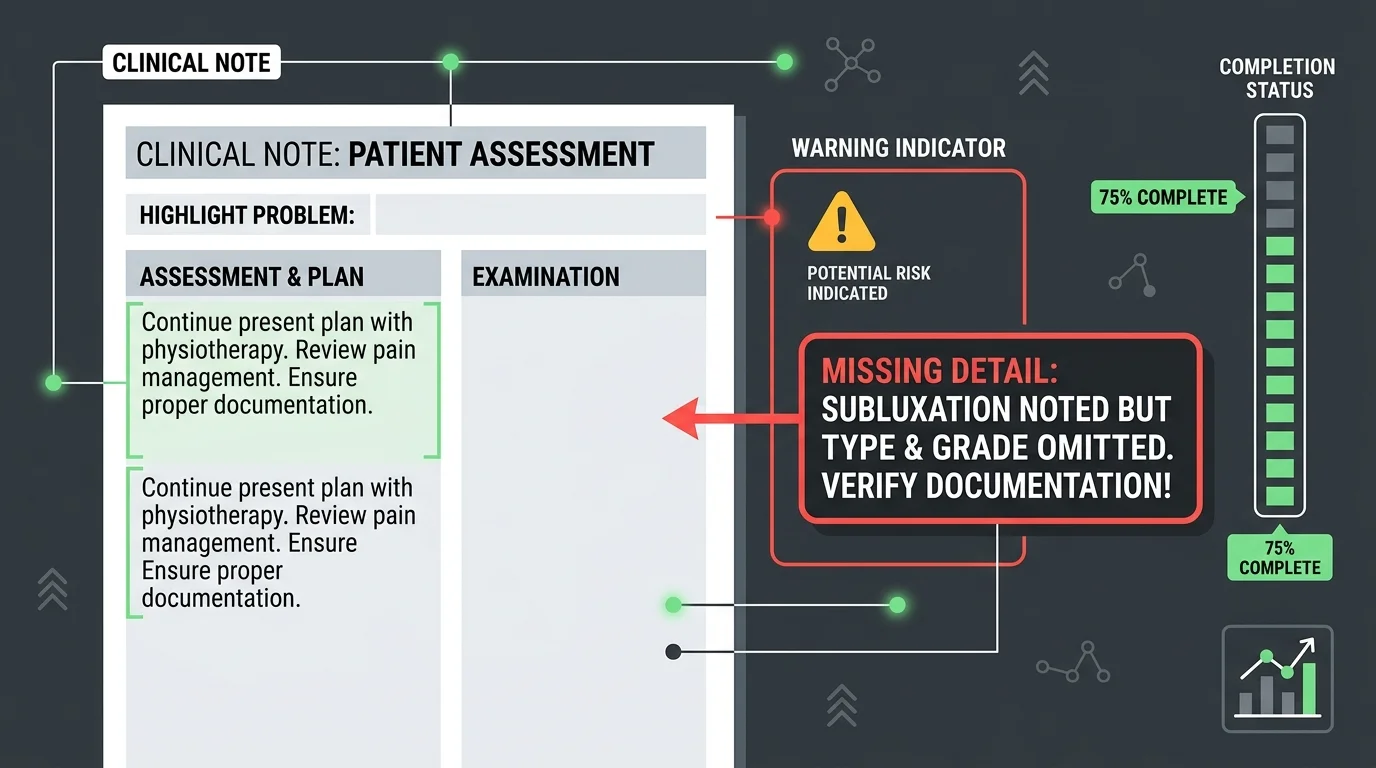
The documentation problem compounds the coding problem. EHR template cloning — where clinical notes are copied or auto-populated from a prior session — generates identical records across independent visits. Payer audit algorithms flag that pattern. When a claim is pulled for review, a note that reads identically to the note from six weeks prior does not demonstrate individual medical necessity. It demonstrates a software default.
HHS OIG audits of chiropractic Medicare claims have found that up to 82% of reviewed claims did not meet required clinical documentation standards, with automated template copying identified as a primary contributing factor. The liability for those errors stays with the provider, not the software vendor. Local Coverage Determinations are explicit: modifier codes applied without documenting the exact active treatment phase constitute non-compliant billing.
In 2026, with Medicare audit scrutiny intensifying, the question is not whether the auto-coder submits claims quickly. The question is whether every modifier applied to every Medicare claim reflects a clinically verified, individually documented treatment decision — or a software assumption.
Last Updated: June 22, 2026
- • What EHR Auto-Coders Actually Do — And What They Were Built For
- • Where the Algorithmic Defaults Break Down for Chiropractic
- • How CMS and OIG Identify Auto-Coded Claims in 2026
- • The Documentation Patterns That Trigger Chiropractic Audits
-
• Frequently Asked Questions About EHR Auto-Coder Audit Risk
- • How do EHR auto-coders trigger Medicare audits in 2026?
- • What are the compliance risks of using automated AT modifier mapping?
- • Can I be held liable under the False Claims Act for EHR auto-coder errors?
- • How does a human-led billing process prevent chiropractic audits?
- • What should I do if my auto-coding software has created template duplication?
- • Speed Is Not a Compliance Strategy
What EHR Auto-Coders Actually Do — And What They Were Built For
EHR auto-coders were built to solve one problem: speed. They read diagnosis codes, pull from configuration tables, and push claims out the door faster than any human team.
That speed is the product. It is also the trap.
The same logic that accelerates submission strips out the one thing Medicare actually audits: proof that each code reflects a verified clinical decision on that specific date of service.
Auto-coders were never designed to evaluate clinical nuance. They were designed to move paper. That distinction is exactly why chiropractic specialty billing demands a fundamentally different model.
The Submission Engine Problem
A submission engine measures success by claims volume. How many exit the practice per day. Not whether each claim survives a payer's medical necessity review.
CMS Local Coverage Determinations are direct on this point: the AT modifier maps only after manual affirmation of subluxation and active care treatment necessity. An auto-coder cannot make that affirmation. It applies the modifier because the configuration says to — not because the documentation actually supports it for that patient, on that date, at that treatment phase.
That gap is not a bug. It is a design feature.
The system was never asked to protect your practice from audit exposure. It was asked to get claims out the door.
Why Automation Was Never Designed for Chiropractic Compliance
Chiropractic billing under Medicare sits inside one of the narrowest compliance frameworks in all of healthcare. This is not a general billing environment where a miscoded modifier gets caught and corrected in a follow-up. The AT modifier alone requires treatment-phase awareness — acute versus chronic, corrective versus maintenance — that no general-purpose algorithm delivers reliably at scale. The software doesn't know where your patient is in their care plan. It knows what box was checked in setup.
EHR template cloning makes the exposure worse. When clinical notes auto-populate from a prior session, you end up with identical documentation across independent visits. NIH research confirms that payer audit algorithms are built to flag exactly that pattern. When a claim gets pulled for review, a copied note doesn't demonstrate individual medical necessity — it demonstrates a software default. That's not a documentation gap. That's audit evidence. stay ahead of 2026 regulatory changes
Chiropractic compliance requires specialty-level judgment. AT modifier mapping, maintenance versus active care distinctions, subluxation documentation standards that shift by treatment phase — these aren't general billing skills. They're the exact areas where auto-coding logic breaks down. And they're the exact areas where human-embedded oversight is the only thing that holds up when an auditor comes looking.
| Function | What Auto-Coders Do | What Compliance Requires | The Gap |
|---|---|---|---|
| AT Modifier Assignment | Applies modifier based on software configuration and diagnosis code patterns | Manual affirmation that subluxation and active corrective treatment are documented for that specific date of service | Auto-coder applies what the configuration expects — not what the clinical record proves |
| Treatment Phase Distinction | Processes claims without distinguishing active care from maintenance therapy | Each claim must reflect the patient's current treatment phase — maintenance therapy is categorically excluded from Medicare coverage | Auto-coder cannot distinguish phases; it maps codes uniformly across a patient's full claim history |
| Clinical Note Generation | Auto-populates or clones documentation from prior sessions to accelerate workflow | Each visit note must independently demonstrate individual medical necessity for that encounter | Identical notes across independent visits fail individual necessity reviews and are flagged by payer audit algorithms |
| Subluxation Documentation | Accepts template-driven subluxation entries without verifying clinical specificity per visit | Subluxation must be individually documented with clinical findings that support necessity on each date of service | Template-generated subluxation entries read as software defaults, not as verified clinical decisions |
| Audit Liability | Generates billing output and moves claims to submission — no review of downstream compliance exposure | Provider bears full liability for every modifier applied and every code submitted, regardless of software involvement | Speed of submission does not transfer liability — the practice owns every claim the software generates |
| Performance Metric | Measures success by claim volume and submission throughput per day | Compliance measures success by whether each claim can survive a payer's medical necessity review | Optimizing for throughput and optimizing for audit survival are structurally opposite objectives |
Where the Algorithmic Defaults Break Down for Chiropractic
Auto-coding logic doesn't evaluate clinical reality. It evaluates configuration settings. What gets mapped is whatever the software was built to map — not what your documentation actually says on that specific date of service.
Chiropractic coding under Medicare isn't a general billing problem. It's a specialty-specific compliance problem. The rules around modifier assignment, treatment phase documentation, and subluxation standards are narrow. One wrong assumption baked into the auto-coder's configuration doesn't create one bad claim. It creates the same bad claim — repeated across every date of service the system touches.
That's the cost the practice absorbs — not the software vendor.
The AT Modifier Is Not a Default — It Is a Clinical Judgment
The AT modifier is the most scrutinized billing element in chiropractic Medicare claims. CMS is explicit: it maps only to active, corrective treatment where subluxation and medical necessity have been manually affirmed. That affirmation cannot be automated. It requires a human to read the clinical record for that date of service and confirm the documented findings support active-care status — not maintenance, not routine, not templated.
Auto-coders skip that confirmation step entirely. They apply the modifier because the configuration tells them to. The result is modifier assignment that might be factually correct some of the time — and non-compliant every time the documentation doesn't individually support it. Local Coverage Determinations are not ambiguous: applying modifier codes without documenting the exact active treatment phase is non-compliant billing. Practices in that position aren't dealing with a software settings question. They're dealing with a compliance question — and that's exactly why understanding how AT modifiers map correctly is the starting point.
There's a difference between a correct modifier and a defensible one. Correct means the code was applied. Defensible means the documentation proves why it was. Auto-coders only deliver the first.
Template Cloning and Why Identical Notes Are an Audit Red Flag
Clinical note cloning is one of the most flagged patterns in payer audit algorithms. When EHR software pulls a prior session forward — diagnoses, findings, treatment descriptions — it generates documentation that looks identical across independent clinical visits. Payer audit systems are built to surface exactly that pattern. And when they find it, the practice has no credible defense that each visit was independently evaluated.
Published compliance analysis confirms that template-driven documentation creates systematic audit exposure — specifically because it can't demonstrate what Medicare requires: that medical necessity was individually evaluated on that date of service. A copied note doesn't prove the patient needed treatment that day. It proves the software had a template. Those are not the same thing, and auditors know the difference.
When a claim is pulled for retrospective review and the supporting documentation reads identically to five prior visits, there's no defense. The provider's clinical judgment didn't create that problem. The billing tool did. But the provider is the one who answers for it.
Maintenance Care Versus Active Care — The Distinction Auto-Coders Cannot Make
Medicare doesn't cover maintenance therapy for chiropractic services. That exclusion is categorical — no exceptions, no gray area. Active care and maintenance care are distinct treatment phases, and the billing applied to each must reflect that distinction on every single claim.
Auto-coders don't make treatment-phase distinctions. They process what the system sends. If the EHR is configured to apply active-care codes by default, those codes appear on claims regardless of what the clinical record actually documents. The AT modifier maps to acute or chronic subluxation stages — not to every appointment on the calendar. When the auto-coder can't read that difference, it doesn't pause. It submits.
That's the gap that turns submission speed into audit exposure. A claim exits the practice in seconds. It can still be the wrong claim. And in a Medicare audit, the wrong claim — submitted consistently, across months of billing — isn't a rounding error. It's a pattern. Patterns are what auditors are paid to find.
| Coding Decision | Auto-Coder Default Behavior | CMS/LCD Requirement | Audit Exposure Level |
|---|---|---|---|
| AT Modifier Assignment | Applied automatically based on system configuration — no per-claim clinical review | Must be mapped only after manual affirmation of subluxation and active care treatment necessity on that specific date of service | High — systematic non-compliant modifier use across all Medicare claims |
| Active vs. Maintenance Care Distinction | No treatment-phase evaluation — active-care codes applied by default regardless of clinical context | Billing must reflect the documented treatment phase, claim by claim — maintenance therapy is categorically excluded from Medicare coverage | High — incorrect phase coding triggers retrospective recovery audits |
| Subluxation Documentation | Pulled forward from prior session templates without per-visit clinical verification | Clinical necessity of subluxation must be individually affirmed and documented for each date of service | High — templated documentation fails individual medical necessity review |
| Clinical Note Generation | Auto-populates from prior session records, producing identical notes across independent visits | Each note must demonstrate that medical necessity was individually evaluated on that date — copied notes do not satisfy this standard | High — identical notes across visits are a primary trigger for payer audit algorithms |
| Modifier Code Application Under LCD Rules | Applies modifier codes based on configuration settings, not on documented active treatment phase | Local Coverage Determinations require that the exact active treatment phase be documented before any modifier code is assigned | High — modifier assignment without phase documentation constitutes non-compliant billing |
| Treatment Phase Coding for Acute vs. Chronic Subluxation | No differentiation between acute and chronic subluxation stages — single default code applied across claim types | The AT modifier maps to specific subluxation stages; accurate stage identification requires clinical record review | Moderate to High — undifferentiated coding obscures clinical accuracy and weakens audit defense |
How CMS and OIG Identify Auto-Coded Claims in 2026
CMS and the OIG aren't waiting for a complaint to land on their desk. They've built detection infrastructure specifically designed to surface the patterns auto-coders produce — and they're running it continuously.
Published analysis of HHS OIG provider audits found that up to 82% of audited chiropractic Medicare claims did not meet required clinical documentation standards — with automated template copying identified as a primary driver of that failure rate.
That is not an outlier. That is what happens when submission speed replaces clinical verification as the operating standard.
This starts before a human auditor reads a single note. It starts with data.
The Audit Algorithms Auditors Are Running Against Your Claims
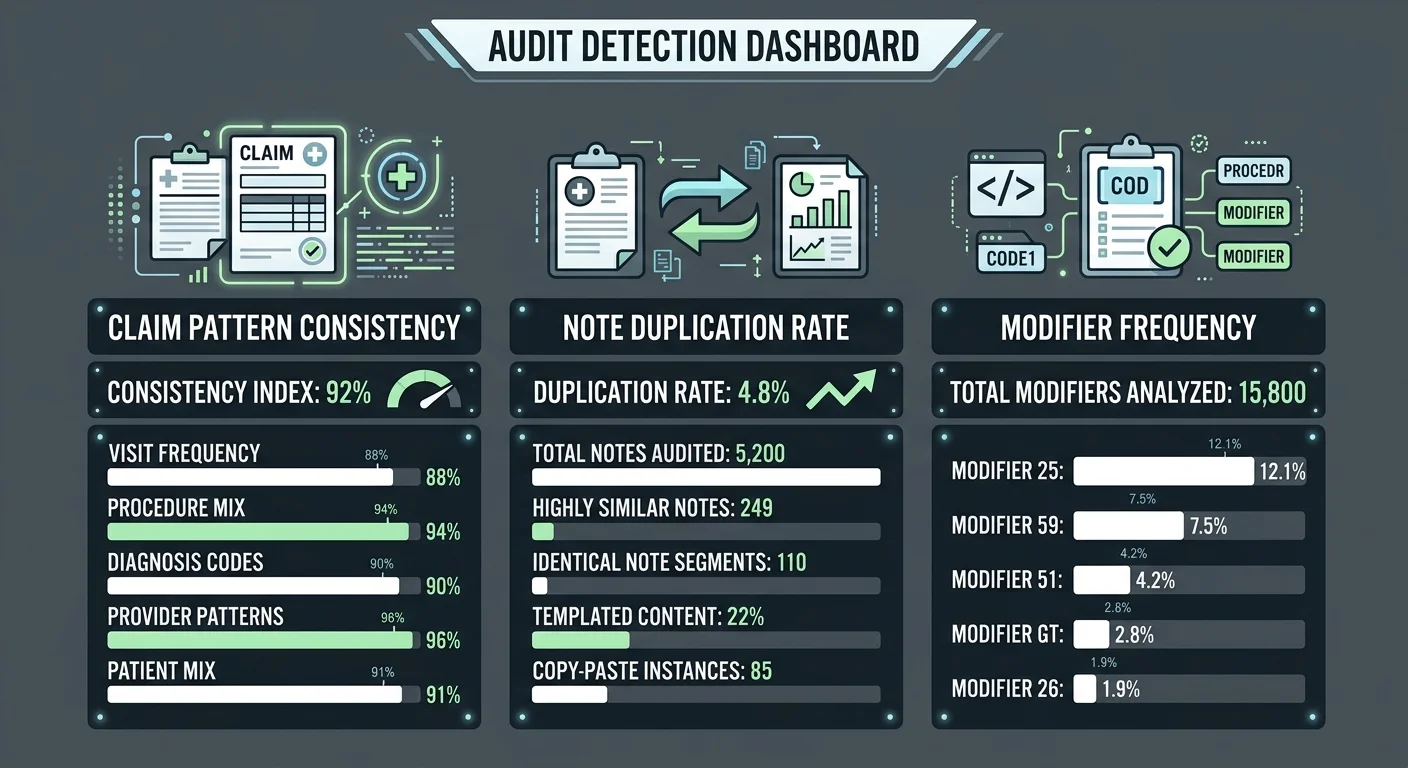
Every Medicare claim moves through algorithmic review before a dollar is released. CMS data systems flag statistical anomalies — modifier usage rates, diagnosis clustering, billing frequency per provider — and surface anything that deviates from expected clinical patterns.
Auto-coded claims reliably produce exactly those anomalies.
When a practice applies the AT modifier at a rate that outpaces the clinical distribution expected for its patient population, that outlier registers. When clinical notes across dozens of claims share identical language, that duplication registers.
These aren't edge cases slipping through cracks. They're the signal the algorithm was built to catch.
An auto-coder optimizes for submission volume. An auditor optimizes for claim defensibility. Those are not the same job — and auditors keep finding the gap.
That gap is exactly what drives the conversation around human intelligence vs. AI coding.
False Claims Act Exposure When Software Generates the Code
Speed doesn't protect a practice from the False Claims Act. The OIG is direct about it: systemic billing and coding errors generated by automated software configurations can expose clinics to federal investigative scrutiny.
The word to hold onto is systemic. That's exactly what auto-coder misconfiguration produces — not a one-off error, but the same wrong answer applied consistently across hundreds of claims.
The software vendor doesn't carry the liability. The provider does. That's not a technicality — it's the OIG's position, stated plainly. When a practice submits hundreds of claims with modifier assignments the documentation can't support, the False Claims Act exposure belongs to the practice. Not to the software configuration. Not to the EHR company. To the doctor who signed off on it.
Compliance analysis from OIG advisory opinions confirms what audit reviews keep finding: the high error rates in chiropractic Medicare claims trace directly back to automated template and coding dependencies — not to one-off human mistakes.
That's the payoff of the speed trap.
The auto-coder moved claims fast. The auditor moved slower — but with full authority to recover every dollar tied to a non-compliant modifier and to refer patterns that cross the False Claims Act threshold.
Submission velocity was never the protection. It was the exposure.
| Audit Trigger | How CMS or OIG Detects It | Likely Consequence | Root Cause in Auto-Coding |
|---|---|---|---|
| AT modifier applied across all Medicare claims | CMS data systems flag modifier usage rates that exceed expected clinical distribution for the provider's patient population | Retrospective claim review; modifier stripped; repayment demand issued | Auto-coder configured to apply AT modifier by default regardless of documented treatment phase |
| Identical clinical notes across multiple dates of service | Payer audit algorithms detect duplicated note language and flag the claim set for manual documentation review | Medical necessity denied for flagged dates; audit expanded to full billing period | EHR template cloning auto-populates prior session notes into new visit records without clinical verification |
| Active-care codes billed during maintenance-phase treatment | OIG cross-references billing codes against treatment frequency and duration patterns inconsistent with active corrective care | Non-covered service determination; full recovery of payments tied to maintenance visits | Auto-coder applies active-care codes by configuration default rather than by treatment-phase documentation |
| Modifier assignment without individual subluxation documentation | CMS Local Coverage Determination review finds modifier applied without the required per-visit clinical affirmation of subluxation and active care status | Claim denied; provider cited for non-compliant billing practices under LCD guidelines | Automated code-mapping skips the manual confirmation step required to link the modifier to that date of service's clinical record |
| Statistically anomalous diagnosis clustering | CMS data systems surface providers whose diagnosis code distribution deviates significantly from peer benchmarks in the same specialty | Provider flagged for targeted audit; all claims in the review period subject to documentation pull | Auto-coder assigns diagnosis codes from a fixed configuration set rather than from individualized clinical findings |
| Systemic billing errors across a high claim volume | OIG identifies patterns consistent with automated software misconfiguration and opens compliance review under False Claims Act standards | Federal investigative scrutiny; liability held by the provider, not the software vendor | High-volume auto-coded output amplifies a single configuration error into a practice-wide compliance failure |
The Documentation Patterns That Trigger Chiropractic Audits
Auditors don't stumble onto problems. They follow patterns. And auto-coders produce those patterns at scale.
OIG audit data puts a number on it: up to 82% of audited chiropractic Medicare claims failed required clinical documentation standards. Automated template copying was the primary driver. That's not a story about bad actors or aggressive billing. That's the baseline result when submission speed is the design goal and no human ever verifies what's actually in the note.
So the question isn't whether your EHR is producing these patterns. It's whether anyone in your billing workflow is catching them before a payer does. That's a different question — and it requires a different kind of review than your software can run on itself. internal coding review
What Reviewers Look for in Chiropractic Clinical Notes
Here's what a reviewer actually does with a chiropractic clinical note: they scan for uniformity. Not clinical quality — uniformity. Identical or near-identical documentation across multiple dates of service is the first thing that draws scrutiny. Every treatment session produces its own findings. If your notes don't reflect that variation, they signal templating. And templating signals that no one was documenting clinical reality — they were filling in a form.
The second pattern is modifier frequency. When the AT modifier appears at a rate that doesn't match the expected clinical distribution for that patient population, it registers in CMS data systems. Local Coverage Determinations are unambiguous: the modifier must map to a documented active treatment phase — acute or chronic subluxation — on every individual claim it touches. Applying it across the board isn't a configuration shortcut. It's a compliance failure. And payer algorithms are specifically designed to detect that frequency outlier.
The third pattern is treatment-phase documentation that doesn't support the billed code. A reviewer pulling a claim compares the submitted code against the clinical note on that specific date of service. If the note doesn't individually establish medical necessity and active-care status, the modifier has no defense. That's not a judgment call. That's a binary documentation standard. And auto-coders don't check it.
The Maintenance Therapy Exclusion and Why Auto-Coders Routinely Violate It
Medicare's exclusion of maintenance therapy from chiropractic coverage isn't a gray area. There's no partial coverage. No situational carve-out. Manual manipulation is covered when it corrects subluxation in an active treatment phase. The moment care shifts to maintenance, coverage stops — full stop.
Auto-coders don't evaluate treatment phase. They process whatever the EHR configuration tells them to apply. If active-care codes are the default setting — and in most chiropractic EHR builds, they are — those codes appear on every claim. Including visits that any careful reading of the clinical record would classify as maintenance. That's not a billing edge case. That's a systematic overpayment pattern baked into the configuration from day one, generating retrospective recovery exposure on every claim it touches.
This is the mechanism the speed trap exploits. The claim exits the practice in seconds, clears initial processing, and gets paid. Then a retrospective audit reaches back and recovers every dollar tied to a maintenance visit billed as active care. Speed is not safety. The documentation was the protection all along. And the auto-coder never touched the documentation.
| Documentation Element | Compliant Standard | Auto-Coder Typical Output | Risk Verdict |
|---|---|---|---|
| Date-of-service clinical findings | Individualized narrative documenting specific patient response, objective findings, and treatment rationale for that visit | Template-populated default text replicated from prior visit notes with minimal or no session-specific variation | High — identical findings across multiple dates signal templating to retrospective reviewers |
| AT modifier application | Modifier assigned only when clinical record documents an active treatment phase tied to acute or chronic subluxation correction | Modifier applied by default across all Medicare claims regardless of documented treatment phase | Critical — blanket application without phase documentation violates Local Coverage Determination requirements |
| Treatment phase classification | Clear distinction between active/corrective care and maintenance care reflected in both clinical notes and submitted codes | Active-care codes applied uniformly; no system-level logic differentiates corrective from maintenance visits | Critical — maintenance visits billed as active care are subject to full retrospective recovery |
| Medical necessity documentation | Individual evaluation of necessity stated explicitly for each date of service, not carried forward from prior encounters | Necessity language copied or auto-populated from previous notes; no session-specific clinical rationale generated | High — copied necessity language fails the individual-date standard required for Medicare defensibility |
| Subluxation level specificity | Documented subluxation location, severity, and clinical basis recorded per visit with objective clinical findings | Diagnosis codes and subluxation references generated from EHR configuration defaults rather than per-visit clinical assessment | Moderate to High — non-specific or repeated subluxation entries trigger payer pattern-matching algorithms |
| Modifier frequency relative to patient population | AT modifier usage rate reflects the actual clinical distribution of active-care patients within the practice | Modifier frequency driven by system defaults rather than clinical distribution, producing statistically anomalous billing patterns | High — outlier modifier rates are a primary CMS data-system flag for audit selection |
Frequently Asked Questions About EHR Auto-Coder Audit Risk
Most practices don't start with the theory. They start with a trigger — a denial cluster, an audit notice, a conversation with another DC who just got hit. That's where the real questions begin.
These are the questions Bushido Billing hears most from chiropractic practices dealing with EHR-related audit exposure in 2026.
How do EHR auto-coders trigger Medicare audits in 2026?
Auto-coders produce patterns. Patterns are what CMS data systems are built to find.
Unusual AT modifier frequency stands out. Identical clinical notes across multiple visits stand out. When the modifier appears at a rate inconsistent with the expected clinical distribution for a given patient population, that outlier registers — and it registers before a human auditor ever reads a note.
Local Coverage Determinations require individual documentation of active treatment phase for every claim. Auto-coders apply default configurations across the full claim volume. That mismatch is the signal.
The system does not wait for a complaint. It finds the pattern.
What are the compliance risks of using automated AT modifier mapping?
The AT modifier must map to a documented active treatment phase — acute or chronic subluxation — on every individual claim. Blanket application across all Medicare visits violates Local Coverage Determinations. That's not a gray area.
OIG audit findings put the failure rate in plain terms: up to 82% of audited chiropractic Medicare claims did not meet required documentation standards. Automated template copying was identified as a primary driver of that number.
That's not a worst-case projection. That is the documented baseline when automated modifier mapping replaces human verification. The risk is real, it's systemic, and it's already sitting in the data.
Can I be held liable under the False Claims Act for EHR auto-coder errors?
Yes. The OIG is direct on this.
Systemic billing errors generated by automated software configurations can expose clinics to False Claims Act liability. The software vendor doesn't carry that exposure. The practice that submitted the claims does.
When hundreds of claims carry modifier assignments the documentation can't support, that's the pattern the OIG flags for federal investigative scrutiny. The word is systemic — not incidental, not occasional. Systemic is exactly what auto-coder misconfiguration produces by design.
Speed is not safety. And it's not a legal defense.
How does a human-led billing process prevent chiropractic audits?
Every claim is reviewed against the actual clinical record before it leaves the practice. That's the structural difference.
Modifier assignment is verified against the documented treatment phase. Maintenance visits aren't billed as active care. The AT modifier only appears where subluxation is individually affirmed — as CMS requires. That review happens claim by claim, not by default configuration.
No auto-coder checks documentation against clinical reality. A trained human reviewer does. That single step is the difference between a defensible claim and an audit liability that compounds across months of billing.
What should I do if my auto-coding software has created template duplication?
Stop treating it as a software settings problem. It's a compliance exposure.
Template duplication is one of the primary patterns OIG audit algorithms are built to surface. Identical or near-identical documentation across multiple dates of service signals templating — not genuine clinical evaluation. That signal draws scrutiny.
The immediate step is a claim-level documentation review. Compare submitted codes against the actual clinical notes on each individual date of service. Every claim where the documentation doesn't support the modifier needs to be identified before a payer identifies it for you.
This doesn't resolve by updating a configuration. It requires a human reviewer who understands what defensible chiropractic documentation actually looks like — and can tell the difference between a compliant claim and one that only looks compliant until someone reads it carefully.
Speed Is Not a Compliance Strategy
The auto-coder was never your compliance partner. It was a submission engine. Those are not the same job. And the practice that treats them as interchangeable is writing audit exposure into every single claim it sends.
Every failure mode in this article traces back to the same architecture problem. Submission velocity and clinical accuracy pull in opposite directions. An algorithm built for throughput will always cut documentation verification, treatment-phase review, and modifier validation — the exact things that make a claim defensible under retrospective scrutiny. The speed felt like efficiency. To a Medicare auditor, it reads as a pattern.
Practices that work with Bushido Billing aren't trading speed for slowness. They're trading exposure for defensibility. A claim that exits with the right modifier, the right documentation alignment, and the right treatment-phase logic behind it is a claim that survives a retrospective review. That is what compliance actually looks like. Speed is not safety. It never protected a single practice from an auditor who already had the data.
If this article described your practice, you're not dealing with a software quirk. You're carrying audit exposure on claims that already went out. Every auto-coded claim sitting unchallenged in a payer's system is building a pattern — and patterns compound before anyone warns you. That's the conversation Bushido Billing is built for. Not a pitch. A clinical billing review by people who know what defensible chiropractic documentation actually requires — and can tell the difference between a compliant claim and one that only looks compliant until a reviewer reads it. The risk doesn't shrink by waiting.

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet