

What Is the Proper Way to Map AT Modifiers to Avoid 2026 Medicare Denials?
The AT modifier is not a formatting detail. It is a clinical declaration — and Medicare treats it like one.
It must be appended to CPT codes 98940, 98941, or 98942 to signal that the service rendered is active spinal manipulation therapy, not maintenance care. Without it, Medicare denies the claim automatically.
That declaration rests on a narrow statutory boundary. Medicare covers manual manipulation of the spine to correct a subluxation. That is the full scope. Maintenance therapy — care that supports rather than restores function — is explicitly excluded under Section 1862(a)(1)(A) of the Social Security Act. Every AT modifier mapping decision sits on top of that legal line.
To clear that line, the patient file must show a reasonable expectation of recovery or significant functional improvement. The treatment plan must contain specific, measurable functional goals. Not general progress notes. Not visit counts. Not clinician intent. Medicare Administrative Contractors audit against those documentation standards directly.
When documentation falls short, the claim becomes an overpayment. The HHS Office of Inspector General has identified extensive improper Medicare payments to chiropractors — with the root cause consistently traced to missing subluxation documentation and absent active treatment indicators. Chiropractic clinics carry elevated retrospective review risk compared to other outpatient physical medicine providers under Medicare Part B. That risk does not shrink when a practice hands modifier decisions to an EHR auto-coder.
Software applies rules. It cannot make a clinical declaration.
Proper AT modifier mapping requires three human validation steps before each claim line is submitted: confirming documented functional improvement, verifying documentation completeness against Medicare's Local Coverage Determinations, and confirming the modifier is correctly appended to the appropriate CPT code. Practices that skip any one of those steps — or hand all three to an automated system — are not managing their denial risk. They are compounding it.
Last Updated: June 22, 2026
- • What the AT Modifier Actually Means Under Medicare
- • Why EHR Auto-Coders Get AT Modifier Mapping Wrong
- • The Documentation Requirements Medicare Actually Enforces
- • How to Build an AT Modifier Mapping Workflow That Holds Up to Audit
-
• Frequently Asked Questions About AT Modifier Mapping
- • What exactly constitutes active treatment for a Medicare chiropractic claim in 2026?
- • Can my chiropractic EHR auto-coder safely assign the AT modifier?
- • How does Medicare distinguish between active corrective care and maintenance therapy?
- • What documentation must be in the patient file to justify mapping the AT modifier?
- • What are the immediate consequences if a practice improperly maps the AT modifier?
- • Does the AT modifier apply to all chiropractic CPT codes billed to Medicare?
- • The Two-Letter Modifier That Determines Whether Medicare Pays You
What the AT Modifier Actually Means Under Medicare
Before you can map AT modifiers correctly, you need to understand what you're actually signing off on every time you append those two letters to a claim.
The AT modifier is not a formatting detail. It is a clinical statement — one that tells Medicare this visit was active, corrective spinal manipulation intended to restore function, not maintain it. Two letters. One binary outcome: paid or denied.
That distinction matters more right now than it ever has. Documentation scrutiny across chiropractic billing is tightening — and practices that treat the AT modifier as a checkbox are about to find out it was always a gatekeeper. The pattern is already visible in 2026 regulatory changes.
The Legal Foundation Behind Two Letters
Here's the thing: the AT modifier's weight doesn't come from a CMS billing manual. It comes from federal statute. Maintenance therapy exclusions for chiropractic services are legally rooted in Section 1862(a)(1)(A) of the Social Security Act — the same statutory framework that defines what Medicare is permitted to pay for at all.
That law draws a hard line — and it's been there since Section 1862(a)(1)(A) of the Social Security Act was written. Maintenance care — therapy that supports rather than restores — is not a covered Medicare service. Published CMS guidance confirms it: Medicare coverage for chiropractic is limited strictly to manual manipulation of the spine to correct a subluxation. Not adjacent therapy. Not supplemental care. Not anything that keeps a patient comfortable without documented functional progress.
So when a provider appends AT to CPT codes 98940, 98941, or 98942, they are not filling in a form field. They are making a legal declaration — that this visit meets the statutory definition of active corrective care under federal law. That declaration is auditable. And it is the provider, not the EHR, who is accountable when Medicare comes back asking questions.
Why the Active Treatment vs. Maintenance Distinction Is the Real Risk
Denials aren't random. They follow patterns. The dominant pattern in Medicare chiropractic denials is a claim line where the clinical reality — maintenance, ongoing support, pain management without measurable functional progress — does not match the active treatment declaration the AT modifier makes.
That mismatch is where real audit exposure lives. NIH-indexed research confirms the AT modifier must be appended to the correct CPT code for every active treatment claim — and that every claim line submitted without it is automatically denied. But the missing modifier is not the dangerous failure. The dangerous failure is the modifier that shows up when the documentation does not back it up.
That is the distinction most chiropractic billing services do not make clearly enough. The AT modifier on a visit Medicare classifies as maintenance care is not a billing error. It is an improper payment. And improper payments trigger retrospective reviews, recoupment demands, and audit scrutiny that doesn't stop at one claim — it compounds across your entire claim history.
| Care Type | Medicare Coverage Status | AT Modifier Required | Claim Outcome if Misclassified |
|---|---|---|---|
| Active Corrective Care | Covered under Medicare Part B | Required on CPT 98940, 98941, or 98942 | Claim submitted without AT modifier is automatically denied; claim submitted with AT but lacking supporting documentation triggers recoupment upon review |
| Maintenance Therapy | Explicitly excluded under Section 1862(a)(1)(A) of the Social Security Act | Not applicable — the visit itself is non-covered | AT modifier applied to a non-covered maintenance visit constitutes an improper payment and elevates retrospective audit risk across the entire claim history |
| Supportive or Palliative Care | Not covered — supportive care does not meet the statutory definition of active spinal manipulation to correct a subluxation | Not applicable | Misclassifying supportive care as active treatment produces the same improper payment exposure as maintenance therapy misclassification |
| Active Treatment Without Documented Functional Progress | Conditionally covered — coverage depends on documented evidence of measurable functional improvement, not clinician intent | Required, but insufficient alone | AT modifier present does not protect the claim if the clinical record does not demonstrate a reasonable expectation of recovery or measurable progress toward specific functional goals |
| Active Treatment With Complete Documentation | Covered — all Medicare coverage criteria are met when documentation confirms subluxation, active corrective intent, and measurable functional improvement trajectory | Required and defensible | Claim is payable and audit-defensible; the AT modifier declaration is backed by a clinical record that withstands Medicare Administrative Contractor review |
Why EHR Auto-Coders Get AT Modifier Mapping Wrong
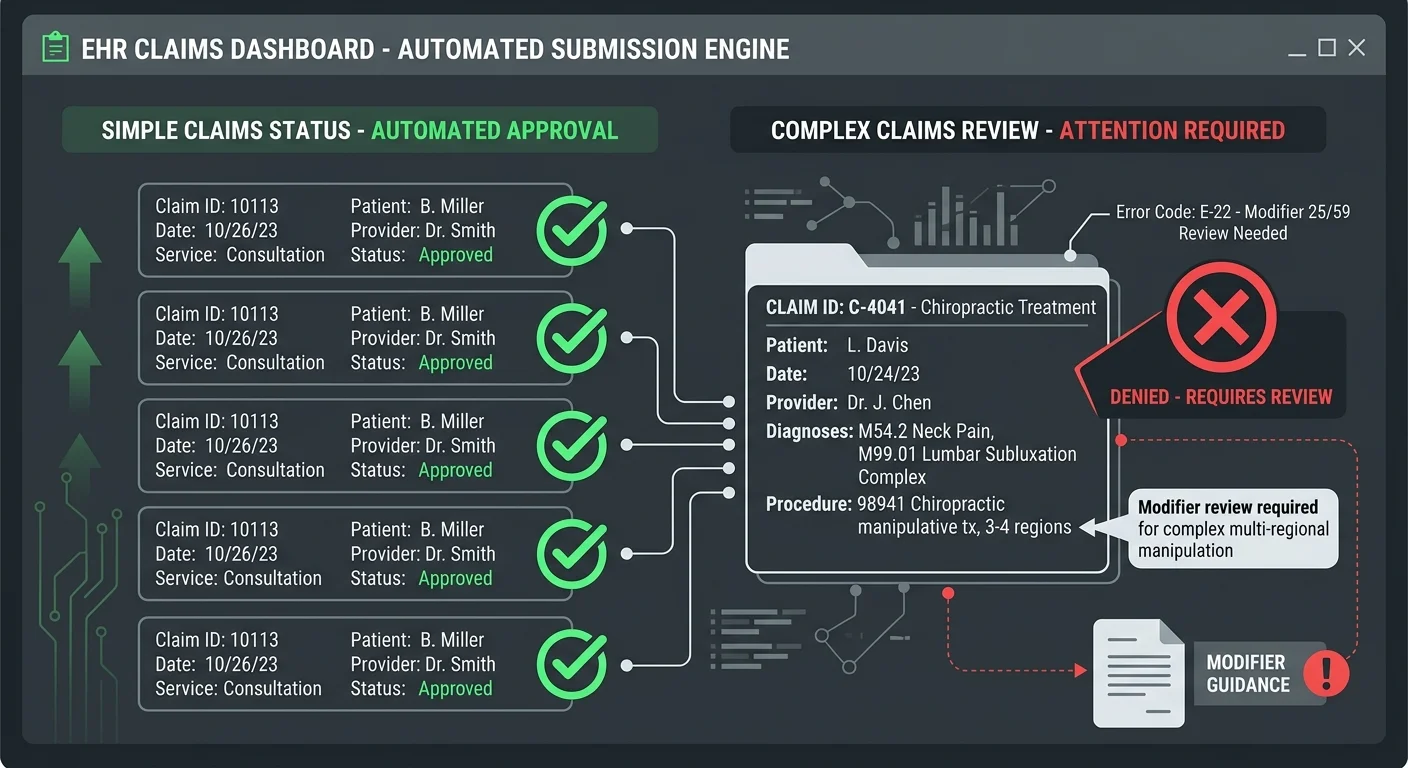
Here's where practices actually lose claims — not in an audit hearing. In the moment an EHR auto-coder silently appended AT to a CPT code without reading a single line of the patient's chart.
EHR software is a submission tool. It processes visit type, CPT code, payer assignment — and it moves on. What it cannot do is read whether the patient's documented functional trajectory on that specific date actually supports a declaration of active corrective care under Medicare's Local Coverage Determinations.
That gap is exactly where EHR auto-coder audit risk compounds. Chiropractic clinics already carry elevated retrospective review risk compared to other outpatient physical medicine providers under Medicare Part B. Handing modifier decisions to an algorithm does not reduce that risk. It amplifies it.
What Auto-Coding Software Is Actually Doing to Your Claims
Here's the thing: auto-coding logic is built around rules, not clinical judgment. It sees a chiropractic manipulative treatment CPT code and a Medicare payer, and it applies the AT modifier — because that is the rule for active treatment claims. It does not ask whether the visit note demonstrates measurable functional improvement. It does not cross-reference the patient's treatment plan goals. It applies the modifier and moves the claim to the submission queue.
That process works — until it doesn't. Clean claims with strong documentation get paid. But the moment a patient's functional progress plateaus, or a visit note contains language Medicare reads as maintenance rather than active restoration, the auto-coder still appends AT. It has no mechanism to detect the difference.
So the claim goes out with the modifier. Medicare processes it. And sometime later — during a retrospective review — an auditor reads that visit note and sees what the software couldn't: the documentation does not support active corrective care. NIH-indexed research confirms that systemic billing errors persist in chiropractic practices without expert management, and the HHS OIG has identified extensive improper Medicare payments to chiropractors traced directly to missing subluxation documentation and absent active treatment indicators. The modifier was there. The clinical support wasn't. That is not a billing error. That is an improper payment.
The Volume-First Model and the Modifier It Can't Read
The volume-first billing model was built around throughput. Submit fast, submit often, work denials reactively. That holds up for clean claims — no modifier ambiguity, no documentation gaps. It breaks down entirely when a claim requires a human to evaluate clinical narrative before deciding whether AT belongs on that visit.
The AT modifier is always a clinical narrative decision. Every chiropractic manipulative treatment claim submitted without it is automatically denied by Medicare. Every claim submitted with it that doesn't survive documentation review becomes an improper payment that triggers recoupment. There is no neutral outcome. The modifier is either defensible or it isn't — and a volume-first model never stops to make that call.
That's the failure the chiropractic EHR billing software conversation almost never surfaces. Services built for high-volume submission optimize for speed. The AT modifier requires the opposite — a deliberate pause before each claim line to run the Functional Improvement Check, the Documentation Completeness Check, and the Claim-Line Modifier Confirmation. Volume models don't budget for that pause. So it disappears. And the audit exposure grows.
Who This Is Not For
Human-gated modifier validation before every claim is not for every practice. If the goal is a fully automated workflow — claims moving from EHR to clearinghouse with no human review of clinical documentation — Bushido Billing is not the right partner.
And if the primary question is cost per claim rather than defensibility per claim, this conversation ends here. Practices comfortable with auto-coder AT mapping — and the retrospective review risk that comes with it — don't need what human-expert validation provides. But practices that have already received a recoupment demand, or watched their Medicare denial rate climb without a clear explanation, know exactly what that automation gap cost them.
| What EHR Auto-Coders Do | What Medicare Actually Requires | The Gap That Creates Denials |
|---|---|---|
| Detects a chiropractic manipulative treatment CPT code (98940, 98941, or 98942) paired with a Medicare payer and applies the AT modifier automatically based on visit type | Requires that the AT modifier reflect a clinical determination — that the service rendered was active, restorative spinal manipulation with documented functional improvement, not supportive maintenance care | The modifier is applied to the rule match, not to the clinical reality of that visit — creating a declaration Medicare can later contradict with the visit note |
| Processes visit data at the point of submission without reading the patient's narrative documentation or treatment plan progress notes | Requires that the patient file demonstrate measurable functional goals and documented progress toward those goals as defined by Medicare Local Coverage Determinations | The Functional Improvement Check never runs — claims move to the submission queue regardless of whether the documentation supports active corrective care status |
| Applies consistent modifier logic across all claims in the submission queue, optimizing for speed and throughput | Requires claim-by-claim evaluation of whether the patient's functional trajectory on that specific date of service crosses the active-versus-maintenance threshold | No deliberate pause exists before submission — the Documentation Completeness Check and Claim-Line Modifier Confirmation are skipped entirely in a volume-first workflow |
| Flags missing modifiers as errors but cannot flag a modifier that is present but clinically unsupported — the system sees a complete claim line and clears it | Requires that every appended AT modifier be defensible under retrospective review — meaning the documentation, not just the code, must satisfy the active treatment standard | A modifier that passes the software's validation logic can still represent an improper payment if an auditor's clinical read of the visit note contradicts the active treatment declaration |
| Treats AT modifier mapping as a formatting and code-matching task that can be resolved with rule-based automation | Treats the AT modifier as a legal declaration under federal statute that requires human clinical judgment to make accurately on each claim line | The gap between a formatting task and a legal declaration is exactly where retrospective audit exposure accumulates — and where systemic billing errors persist without expert management |
The Documentation Requirements Medicare Actually Enforces
Knowing what your software gets wrong is a start. But that's not the problem Medicare is focused on.
Medicare isn't checking your modifier. It's checking whether your file backs it up. Those are two different reviews — and most practices are only ready for one of them.
Medicare Administrative Contractors don't audit for the presence of the AT modifier.
They audit whether the documentation in your patient file actually supports the declaration that modifier makes. Most practices are prepared for the first question. Almost none are prepared for the second.
The 2026 ICD-10 SDOH updates have sharpened documentation scrutiny across chiropractic Medicare billing. But the AT modifier documentation requirements aren't a 2026 invention.
They've been embedded in published administrative guidance for years. Specific. Measurable. Non-negotiable. What changed in 2026 is how aggressively contractors are applying them.
What Must Be in the Patient File on Every Claim Date
Medicare doesn't evaluate a chiropractic visit in the abstract.
It evaluates what's written in your file on that specific date — against a defined standard. Not your intent. Not your clinical judgment. What's documented.
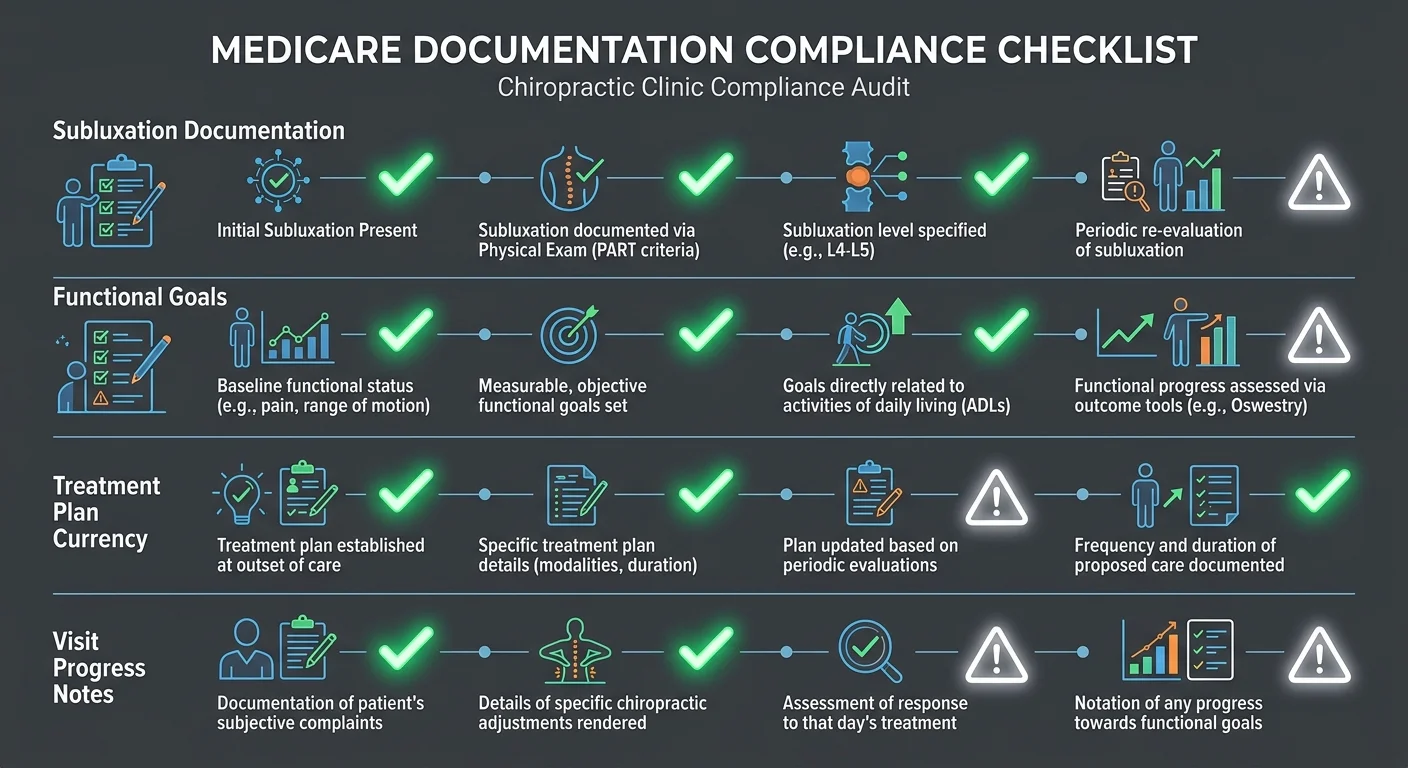
That standard requires a treatment plan with specific, measurable functional goals. Not general improvement. Not patient-reported pain reduction.
Range of motion. Activities of daily living. Objective findings that show the patient has a reasonable expectation of recovery or meaningful functional advancement. Every claim date the AT modifier appears has to connect back to documentation that moves that functional story forward. If the notes don't advance the narrative, the modifier doesn't hold.
Medicare coverage itself is constrained by statute. Coverage is limited to manual manipulation of the spine to correct a subluxation. Maintenance therapy — care that supports rather than restores — is not a covered service.
this published analysis traces that exclusion directly to Section 1862(a)(1)(A) of the Social Security Act. The documentation has to show active restoration. Not ongoing support. Not symptom management.
The line between those two is exactly where auditors spend their time.
How Medicare Auditors Evaluate Functional Improvement
Medicare auditors are not reading visit notes looking for the AT modifier.
They are reading for evidence that the patient's documented functional status on that date supports active corrective care — and for the presence of language that signals the visit has shifted into maintenance territory.
The Functional Improvement Check isn't a formality.
Auditors look for objective, measurable indicators of progress toward the goals stated in the treatment plan. When those indicators are absent — when a visit note reads as routine, supportive, or pain-management-focused without documented functional advancement — the AT modifier on that claim line becomes indefensible.
That's how the audit gap widens. Not from a single bad claim. From months of claims going out the same way, with no one catching the pattern.
Practices that understand this audit dynamic build documentation review into every claim — not as a compliance box, but as a revenue protection discipline.
Because the pattern never changes: the modifier was applied, the visit note didn't support it, and by the time the recoupment demand arrived, months of claims had already gone out the same way.
That's not bad luck. That's what happens when no one is reviewing documentation before the claim goes out.
| Documentation Element | Medicare Requirement | Common Deficiency | Audit Outcome if Missing |
|---|---|---|---|
| Treatment Plan Goals | Must outline specific, measurable functional goals — range of motion, activities of daily living, documented objective findings | Vague improvement language; patient-reported pain reduction without objective benchmarks | AT modifier on every associated claim line becomes indefensible; auditor classifies care as maintenance |
| Expectation of Recovery | Documentation must support that the patient has a reasonable expectation of recovery or significant functional improvement | No documented functional trajectory; visit notes read as routine or supportive without measurable advancement | Claim reclassified as maintenance therapy; recoupment demand issued for all affected dates |
| Active vs. Maintenance Distinction | Documentation must demonstrate active restoration — not ongoing supportive care — on each specific claim date | Visit note language that is supportive or pain-management-focused without functional advancement indicators | Auditor finds care consistent with maintenance therapy; AT modifier disqualified under statutory exclusion |
| Subluxation Documentation | Medicare coverage is limited strictly to manual manipulation of the spine to correct a subluxation — subluxation must be documented | Missing or incomplete subluxation documentation; no objective clinical finding recorded to support manipulation | Claim denied outright; no AT modifier can rescue a claim lacking the foundational coverage criterion |
| Maintenance Therapy Exclusion | Maintenance therapy is not a covered service under Medicare — documentation must affirmatively show care is not maintenance | No explicit distinction in the visit note between active corrective treatment and ongoing supportive management | Medicare applies the statutory exclusion under Section 1862(a)(1)(A); all claims for that patient period subject to recoupment |
How to Build an AT Modifier Mapping Workflow That Holds Up to Audit
Knowing what Medicare requires is the easy part. Getting it right on every claim, every visit, every billing cycle — that's the actual problem.
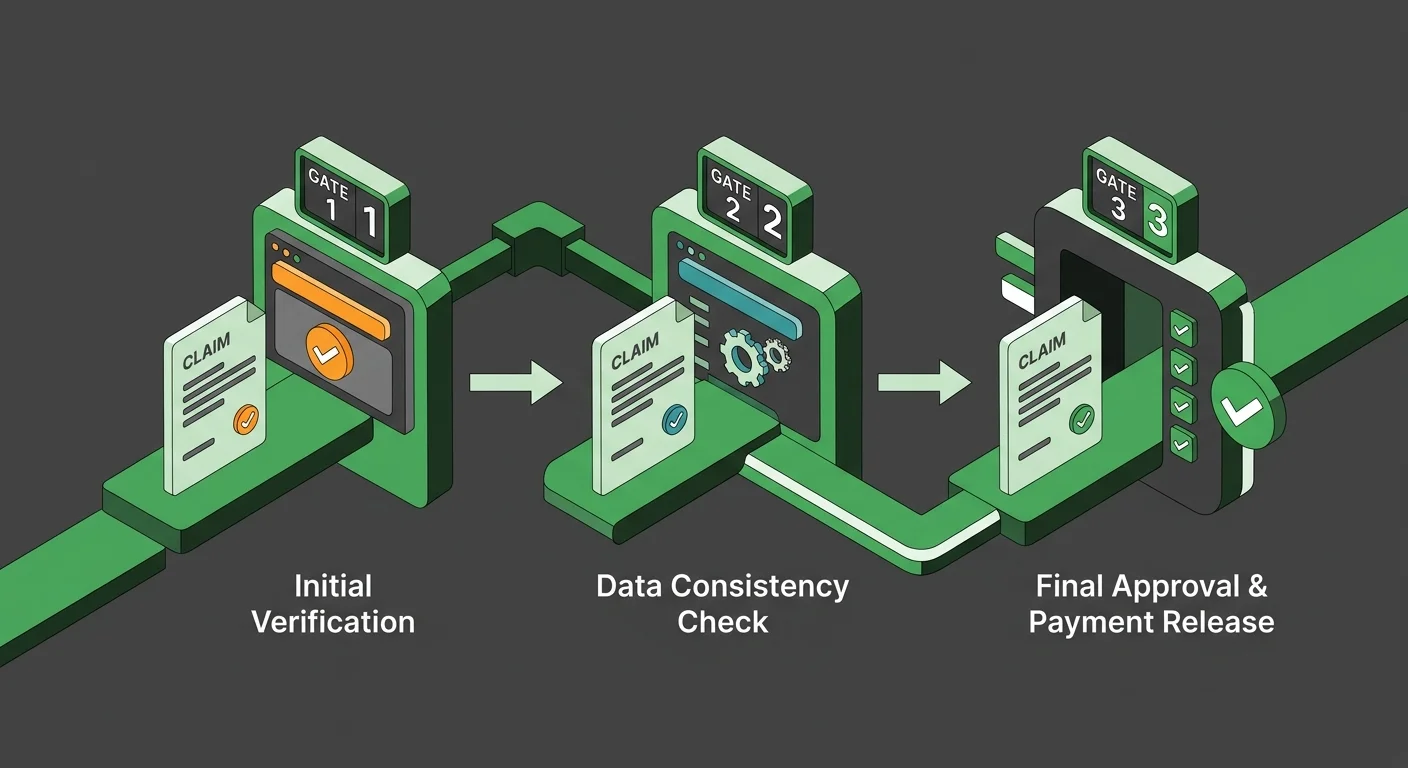
The AT modifier workflow that holds up to audit runs three sequential validation gates before any claim line reaches the submission queue: the Functional Improvement Check, the Documentation Completeness Check, and the Claim-Line Modifier Confirmation.
Each gate has a pass condition. If a claim does not clear all three, the modifier does not go on the claim.
That's the whole structure. Deliberate, sequential, and non-negotiable.
Gate, evaluate, confirm. That sequence is what separates a defensible AT modifier from an auto-applied one — and what separates practices that survive retrospective review from the ones untangling recoupment demands six months later. Build this process before the denial letter arrives. The practices that wait build it under duress, with fewer clean options. coding review before regulatory pressure arrives
Validation Gate 1: Functional Improvement Check
Gate 1 asks one question: does today's visit note show measurable functional improvement toward the goals in the active treatment plan? If the answer isn't clearly yes, the gate doesn't open.
Medicare Administrative Contractors require a treatment plan with specific, measurable functional goals to justify active corrective care status. The Functional Improvement Check verifies that the visit note on the claim date actually advances that functional narrative — objective findings, range of motion data, documented activities-of-daily-living changes that show a reasonable expectation of recovery or significant improvement.
General pain reduction language does not pass this gate.
Routine maintenance language does not pass this gate.
So if the visit note reads as supportive or palliative rather than restorative, Gate 1 fails. The AT modifier does not go on that claim.
That call cannot be automated. It requires someone who has read the file, understands the patient's trajectory, and knows the difference between a visit that advances a functional goal and one that maintains a baseline.
Software applies rules. It cannot make a clinical declaration. Those are not the same thing.
Validation Gate 2: Documentation Completeness Check
Gate 2 is not a spelling check. It's a structural audit — confirming the claim file contains every element Medicare looks for when it pulls that claim for review. One missing piece is enough to turn a legitimate claim into an improper payment finding.
HHS OIG audits have repeatedly traced Medicare overpayments to chiropractors back to the same root cause: missing subluxation documentation and absent active treatment indicators. Not fraud. Missing paperwork.
The Documentation Completeness Check exists to close that gap before submission. It confirms the file contains: a current treatment plan with measurable goals, an initial or updated subluxation diagnosis, objective clinical findings from the date of service, and visit notes that connect that date's care to the functional restoration trajectory.
And Gate 2 runs before the claim is submitted. That timing is the whole point.
HHS OIG-identified improper payments were largely attributed to documentation failures that a pre-submission review would have caught. Reactive denial management finds the problem after the claim has already been paid, reviewed, and potentially recouped. At that point, the options are limited and the revenue is already at risk.
Pre-submission review finds the problem while there's still time to fix it.
Validation Gate 3: Claim-Line Modifier Confirmation
Gate 3 is the claim-line confirmation: is the AT modifier correctly appended to CPT code 98940, CPT code 98941, or CPT code 98942 — and only those codes — on this specific claim line?
Every chiropractic manipulative treatment claim submitted without the AT modifier is automatically denied by Medicare. But Gate 3 is not just checking presence.
Presence without support is an improper payment waiting to be found. Gate 3 verifies that the modifier on that claim line is backed by what Gates 1 and 2 actually reviewed. If the documentation doesn't hold, the modifier doesn't go on — regardless of what the EHR defaulted to.
That's the complete circuit. The Functional Improvement Check establishes clinical justification. The Documentation Completeness Check confirms the file supports that justification. The Claim-Line Modifier Confirmation locks the modifier to the code — only after the first two gates have cleared.
Run all three in sequence on every Medicare chiropractic claim, and the AT modifier on that claim is not a guess.
It is a defensible declaration.
| Validation Gate | What Is Checked | Who Performs the Check | Consequence of Skipping |
|---|---|---|---|
| Functional Improvement Check | Does the visit note demonstrate measurable functional progress — objective findings, range of motion data, or documented activities-of-daily-living changes — toward the goals in the active treatment plan? | Human billing reviewer with clinical context — requires reading the patient file and understanding the functional trajectory, not running an automated rule | AT modifier is applied to a visit that Medicare classifies as maintenance or supportive care — the claim becomes indefensible under retrospective audit scrutiny |
| Documentation Completeness Check | Does the claim file contain every structural element Medicare requires: a current treatment plan with measurable goals, a subluxation diagnosis, objective clinical findings on the date of service, and visit notes that connect that date's care to the functional restoration trajectory? | Human billing reviewer cross-referencing the file against Medicare Local Coverage Determination requirements before submission | Claim is submitted with documentation gaps that OIG audits have historically flagged as the primary driver of improper payment findings — gaps that pre-submission review would have caught |
| Claim-Line Modifier Confirmation | Is the AT modifier correctly appended to CPT code 98940, 98941, or 98942 on this specific claim line — and is that modifier supported by the documentation verified in Gates 1 and 2? | Billing specialist performing final claim-line verification after both prior gates have cleared — confirmation of presence and defensibility, not just presence alone | Claim is either automatically denied for a missing modifier or submitted with a modifier that the documentation cannot support — two failure modes with the same audit consequence |
Frequently Asked Questions About AT Modifier Mapping
The rules are written down. Applying them correctly — that's where practices get into trouble.
These are the questions practices ask most. The answers are direct — because the consequences aren't small.
What exactly constitutes active treatment for a Medicare chiropractic claim in 2026?
Active treatment means the patient has a documented, reasonable expectation of recovery or significant functional improvement — and the care on that date is restorative, not supportive.
Medicare covers one thing for chiropractic: manual manipulation of the spine to correct a subluxation. Active treatment, inside that definition, is manipulation directed at correcting a subluxation with measurable functional progress tied to goals in the treatment plan.
The moment care shifts to maintaining a patient's baseline rather than advancing it, that visit is no longer active treatment. It doesn't matter which CPT code is on the claim.
Can my chiropractic EHR auto-coder safely assign the AT modifier?
No.
An EHR auto-coder can confirm that a spinal manipulation happened and attach the AT modifier to CPT 98940, 98941, or 98942. That's it. That's the full scope of what the software does.
It doesn't read the visit note. It doesn't evaluate whether documented findings show measurable functional improvement toward the treatment plan's stated goals. It doesn't determine whether the claim clears Medicare's active corrective care standard. That's a clinical judgment call. Software runs a pattern match.
Those are not the same thing. And Medicare's retrospective review process exists specifically to find that gap.
How does Medicare distinguish between active corrective care and maintenance therapy?
The line is statutory. Section 1862(a)(1)(A) of the Social Security Act defines it: maintenance care is therapy that is supportive rather than restorative, and Medicare does not cover it.
In practice, Medicare Administrative Contractors look at the visit note for objective functional advancement — range of motion improvement, documented activities-of-daily-living gains, measurable progress toward the treatment plan's stated functional goals.
A note that documents pain management, a routine adjustment, or ongoing support without linking it to a functional restoration trajectory is maintenance care under that standard. What the provider intended doesn't factor in. What the documentation says is all that matters.
What documentation must be in the patient file to justify mapping the AT modifier?
What are the immediate consequences if a practice improperly maps the AT modifier?
Two consequences. They are not the same.
A missing AT modifier is an automatic denial. Every chiropractic manipulative treatment claim without it gets rejected by Medicare immediately.
Improper mapping is worse. Applying the AT modifier when the documentation doesn't support active corrective care isn't a billing error — it's an improper payment. Medicare's retrospective review reaches back across multiple billing periods. When auditors find a pattern of AT modifier use that the documentation doesn't support, the result is a recoupment demand covering months of billing the practice already received.
That's what skipping documentation review at the claim level actually costs. Not one denied claim. A demand to return money that's already been spent.
Does the AT modifier apply to all chiropractic CPT codes billed to Medicare?
No. The AT modifier applies only to CPT codes 98940, 98941, and 98942 — the spinal manipulation codes — when billed to Medicare for active corrective care. It doesn't apply to other chiropractic or physical medicine codes.
And it doesn't apply automatically to those three codes either. It applies only when the documentation supports that the visit constitutes active treatment under Medicare's standard. Maintenance therapy billed under the same CPT codes is still not a covered Medicare service.
The modifier on the claim line is a declaration. The documentation is what makes that declaration defensible — or what makes it the centerpiece of a recoupment demand.
The Two-Letter Modifier That Determines Whether Medicare Pays You
The practices getting audited right now didn't ignore the rule.
They trusted software to make the clinical declaration the AT modifier represents. And during retrospective review, they found out no algorithm was ever built to do that.
Medicare doesn't ask what your EHR decided. It asks what the documentation shows. Those are two different questions. Only one has an answer that holds up.
The AT modifier is not a formatting detail. It's a declaration — that the patient receiving spinal manipulation on that specific date had a reasonable expectation of recovery or significant functional improvement. That the care was restorative, not supportive. That the file proves it.
Medicare coverage is limited strictly to manual manipulation of the spine to correct a subluxation. Every claim line carrying the AT modifier on CPT codes 98940, 98941, or 98942 is asserting that this visit met that statutory standard under Section 1862(a)(1)(A) of the Social Security Act.
Software applies rules. It cannot make that assertion.
The Functional Improvement Check, the Documentation Completeness Check, and the Claim-Line Modifier Confirmation exist because that assertion has to be true — not assumed, not auto-applied, and not discovered to be wrong when an auditor pulls the file.
Two letters determine whether Medicare pays or denies. The documentation determines whether those two letters are defensible. And the process — who reviews it, how, and before the claim goes out — determines whether a practice builds a billing operation that holds up under scrutiny or one that only looks clean until an auditor pulls the file.
Bushido Billing was built by people who have run a chiropractic practice. They know what that audit moment costs — in time, in recoupment demands, and in the revenue that doesn't come back.
The answer isn't faster software. It's human expertise that knows the difference between a visit note that advances a functional goal and one that doesn't — before the claim ever leaves the queue.
If your current process can't tell the difference, neither can your defense.
Your documentation either backs that declaration — or it doesn't. A practice assessment shows you exactly where your AT modifier validation breaks down and what it's costing you in retrospective review exposure. Book a Call to find out whether your process can survive scrutiny.

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet