

What Are the Audit Triggers for Unspecified Diagnosis Codes in 2026?
Unspecified diagnosis codes are one of the most reliable audit triggers in chiropractic billing. Payers in 2026 aren't waiting for a human reviewer to find them. Automated claims systems are configured to flag or reject unspecified lateralization codes the moment a specific spinal region or limb is required — the claim never reaches adjudication.
It gets stopped, returned, or queued for scrutiny before anyone at the practice knows what happened.
ICD-10-CM guidelines are direct on this point: unspecified codes are only appropriate when clinical information is genuinely unavailable or non-specific at the time of the encounter. For chiropractic encounters, that threshold is rarely met. The treating provider knows the spinal level. The provider knows the side. When that information exists but doesn't appear in the code, the gap reads as either a documentation failure or a medical necessity problem — and neither is a defensible position.
The stakes are documented. Regional OIG audits found that 82% of chiropractic claims reviewed did not meet Medicare requirements, with documentation deficiencies cited as a primary driver. Peer-reviewed research confirms that failure to document subluxations at specific spinal levels ranks among the top triggers for post-payment audits. A practice still running unspecified codes — by habit, by EHR template default, or by billing workflow shortcut — is building a pattern that retrospective audits are specifically designed to find.
The AT modifier compounds the exposure. CMS guidelines require the AT modifier on chiropractic Medicare claims to demonstrate active corrective treatment rather than maintenance care. When the underlying diagnosis code is unspecified, the AT modifier's medical necessity argument collapses. There is no specific clinical finding to anchor it. The American Chiropractic Association requires active care claims to be supported by quantitative measures of functional improvement — and those measures must tie to a specific, documented condition.
A claim with an unspecified code asks the payer to trust the practice without giving them a reason to. In 2026, eliminating unspecified diagnosis codes is not a coding preference. It is a fundamental requirement for protecting revenue the practice has already earned.
Last Updated: June 22, 2026
- • Why Unspecified Codes Are a Primary Audit Magnet in 2026
- • Why the Volume-First Billing Model Produces Unspecified Codes
- • How Automated Payer Edits Flag Unspecified Codes
- • What Chiropractic Practices Must Change to Eliminate Unspecified Code Risk
-
• Frequently Asked Questions
- • What makes unspecified diagnosis codes an automatic audit trigger in 2026?
- • How do automated payer edits identify chiropractic claims with unspecified codes?
- • What specific clinical scenarios allow for unspecified coding without triggering a denial?
- • How does using an unspecified ICD-10 code impact the AT modifier validation?
- • What steps can chiropractic practices take to audit their own EHR templates for unspecified codes?
- • Coding Specificity Is Not Optional in 2026
Why Unspecified Codes Are a Primary Audit Magnet in 2026
Payers aren't stumbling onto unspecified diagnosis codes. They're finding them on purpose — through automated logic that runs before a human adjudicator ever opens the file.
An unspecified code sends one signal to the payer: the clinical picture wasn't recorded with enough precision to support a targeted diagnosis. For a chiropractic claim, that's not a minor formatting gap. It's the exact pattern audit filters are built to catch. Federal audit data on regional OIG findings puts a number on it — 82% of chiropractic claims reviewed failed Medicare requirements, with documentation deficiencies leading every category of cause.
That failure rate isn't a fluke. It's a structural problem — and unspecified coding is one of the clearest symptoms.
What ICD-10 Specificity Rules Actually Require
ICD-10-CM guidelines are specific: unspecified codes are appropriate only when clinical information is genuinely unavailable or non-specific at the time of the encounter. That's the whole rule. No carve-out for an EHR template that defaulted to an unspecified code. No exception because the provider assumed the extra detail wasn't required. The standard is clear, and auditors apply it without the benefit of the doubt.
For chiropractic practices, meeting the specificity threshold in the CDC guidelines isn't a heavy lift. The treating provider knows the spinal level. The lateralization is documented in the adjustment itself. When that detail lives in the clinical record but never makes it into the submitted code, the gap isn't ambiguous. It's a documentation failure — and payers read it as one.
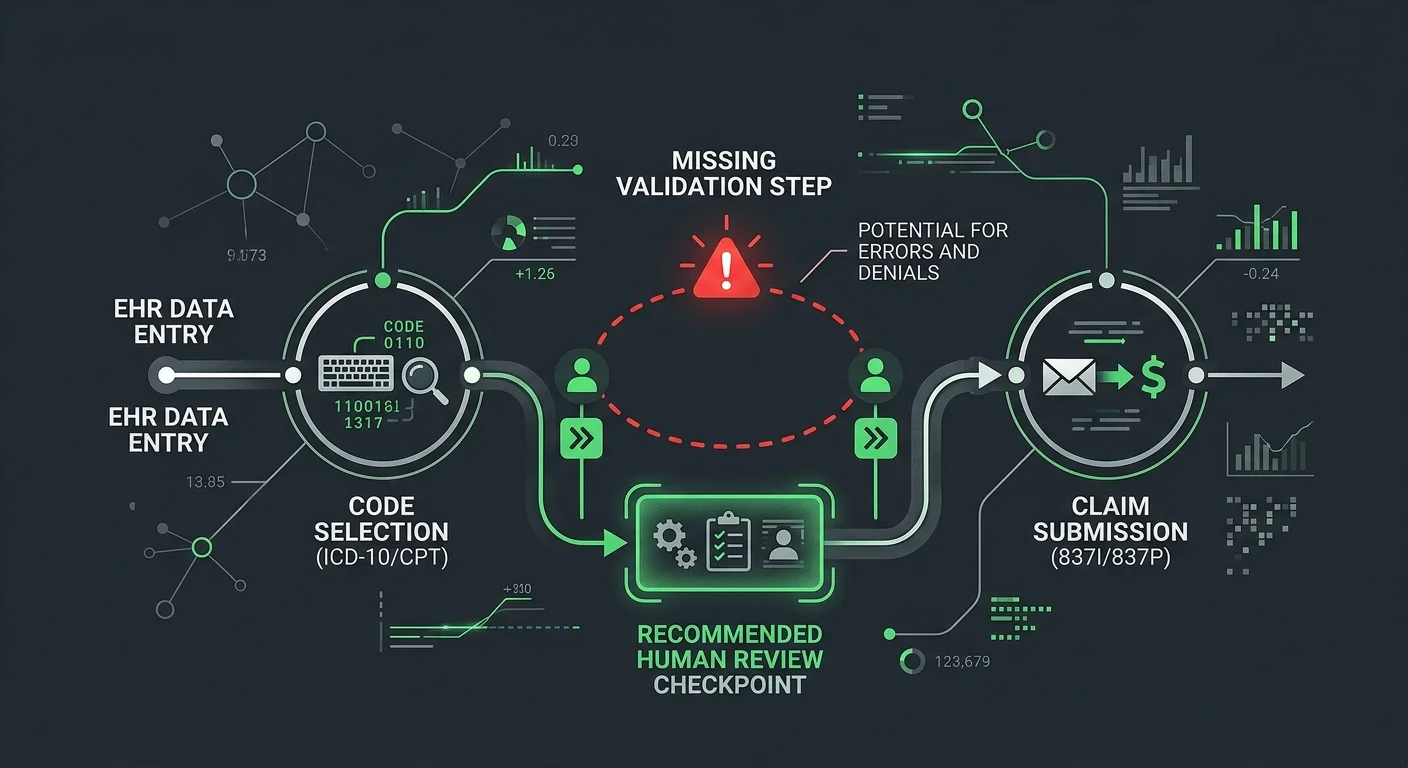
Generic EHR submission workflows weren't built to enforce specialty-level coding specificity. They process what the template produces. When the template defaults to an unspecified code, the system doesn't flag it — it submits it. Catching that gap requires human review at the point of code selection. Not a denial letter three weeks later. 2026 regulatory changes
Why the Absence of Specificity Is Never a Neutral Act
Here's what most coding explanations miss: submitting an unspecified code isn't passive. It's a choice — made by a provider, a biller, or a software default — and payers treat it exactly that way.
A claim with an unspecified code asks the payer to trust you without giving them a reason to. There's no specific anatomical finding anchoring the medical necessity argument. No lateralization confirming the provider treated a documented, identifiable condition. What the payer receives is a claim shaped like a question — and audit systems are built to queue those, not approve them.
That scrutiny compounds. A single unspecified code produces a denial or a records request. A pattern of them — which is exactly what EHR template defaults and high-volume automated workflows generate — builds an audit profile over time. Practices that treat unspecified diagnosis codes as a routine shortcut aren't saving time. They're accumulating exposure with every billing cycle. And the retrospective audit that eventually surfaces that pattern won't distinguish between habit and intent.
| Code Specificity Level | Example ICD-10 Code | Payer Risk Classification | Audit Probability |
|---|---|---|---|
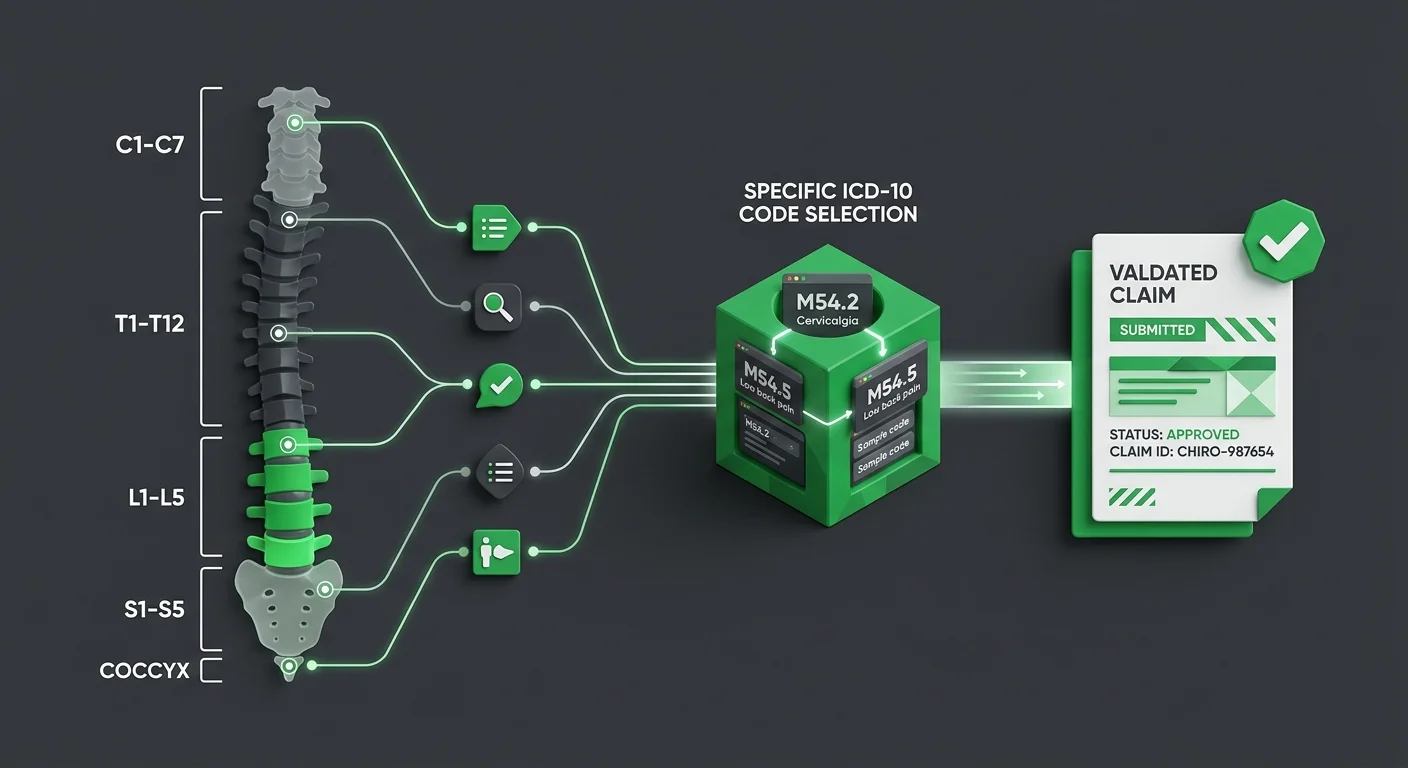
| Fully Specified with Lateralization | M54.42 — Lumbago with sciatica, left side | Low — claim presents complete clinical picture; automated edits pass without flag | Low — specific anatomical documentation supports medical necessity review |
| Specified Region, No Lateralization | M54.5 — Low back pain (without side specified) | Moderate — lateralization gap may trigger edit depending on payer rules and claim history | Elevated — records request likely if claim is part of a pattern; adjudicator may question whether lateralization was available |
| Unspecified Spinal Region | M54.9 — Dorsalgia, unspecified | High — automated payer edits are configured to flag unspecified spinal codes when a region is clinically required | High — signals documentation deficiency; common in retrospective audit profiles built around repeat unspecified billing |
| Unspecified Anatomical Site (Non-Spinal) | M79.3 — Panniculitis, unspecified site | High — unspecified site codes in chiropractic context draw automated scrutiny when a treatable region is expected | High — absence of site specificity collapses medical necessity argument; AT modifier support becomes untenable |
| Placeholder or Default EHR Code | M99.00 — Segmental dysfunction, unspecified region | Critical — generic EHR template defaults are a known audit pattern; payers cross-reference for volume anomalies | Critical — pattern of identical unspecified default codes across multiple encounters is a primary retrospective audit trigger |
Why the Volume-First Billing Model Produces Unspecified Codes
So the audit risk is real and documented. But that still leaves the more important question: why do unspecified codes keep showing up in the first place? It's not carelessness. It's structural.
Here's how volume-first billing actually works: one metric drives everything — submission speed. Clean claims move fast. So the entire workflow gets engineered around clean claims. Clinical specificity — the kind chiropractic billing actually demands — never makes it into that equation.
The workflow runs efficiently. And it quietly generates exactly the documentation gaps that draw payer scrutiny. Unspecified codes aren't random errors. They're the predictable output of a system that was never designed to catch them.
How EHR Templates Automate the Wrong Code
EHR templates are built for speed, not for specificity. When a provider documents a chiropractic encounter, the template often auto-populates the most recent diagnosis code — or defaults to an unspecified code because it fills the required field without demanding any additional input. The provider doesn't have to think about it. That's the whole design. And that's the problem.
The provider treated a specific spinal level at a specific lateralization. That information exists in the clinical record. But when the EHR template never surfaces the specificity requirement at the moment the provider selects a code, the unspecified code enters the claim completely unchallenged. Peer-reviewed research confirms that failure to document subluxations at specific spinal levels is one of the leading triggers for post-payment audits. The clinical reality was documented. The billing reality wasn't.
And the exposure compounds every time a new code category enters the picture. A template that defaults to unspecified doesn't distinguish between established codes and new ones — it just fills the field. Practices already working through expanded coding obligations in 2026 face that exact dynamic with new ICD-10 SDOH codes.
Why Most Billing Workflows Never Catch the Error Before Submission
Most billing workflows have exactly one quality gate: the clearinghouse edit. If the claim clears, it moves. But clearinghouse edits validate claim format. They don't evaluate clinical appropriateness. Those are two completely different things.
So the unspecified code passes through. The claim submits. The biller marks it done. No one caught the error because no step in the workflow was designed to look for it. CMS guidelines require the AT modifier to demonstrate active corrective treatment — and when an unspecified code accompanies that modifier, the medical necessity argument is already compromised before the payer opens the file. Knowing how to document active care with the specificity CMS requires is the exact gap that volume-first workflows consistently fail to close.
That's what CMS guidance on chiropractic documentation errors keeps surfacing: the error isn't caught pre-submission because no one in the workflow was ever assigned to enforce specialty-level coding standards. By the time an audit reveals the pattern, it isn't a single claim problem. It's a billing history problem.
| Workflow Type | Code Selection Method | Specificity Validation Step | Audit Exposure Level |
|---|---|---|---|
| High-volume automated workflow | EHR template default — auto-populates most recent or generic code | Clearinghouse format validation only — no clinical specificity check | High — unspecified codes pass through unchallenged every cycle |
| EHR-integrated billing platform | Software-driven code suggestion based on diagnosis field completion | Automated edit check — validates claim structure, not anatomical detail | High — lateralization and spinal level gaps are invisible to the system |
| Generalist billing service | Coder selects from standard code library without chiropractic specialty review | Single pre-submission scrub — focused on format, not modifier-to-diagnosis alignment | Elevated — AT modifier medical necessity argument remains unsupported |
| Specialty-trained human review | Coder confirms spinal level, lateralization, and diagnosis against clinical documentation | Pre-submission human validation step enforces specificity before claim leaves the practice | Reduced — code selection is anchored to documented clinical findings |
| Embedded chiropractic billing specialist | Code selection driven by clinical record review, not template defaults | Dedicated review of AT modifier alignment with specific, documented active care findings | Minimized — each claim carries a traceable medical necessity argument before submission |
How Automated Payer Edits Flag Unspecified Codes
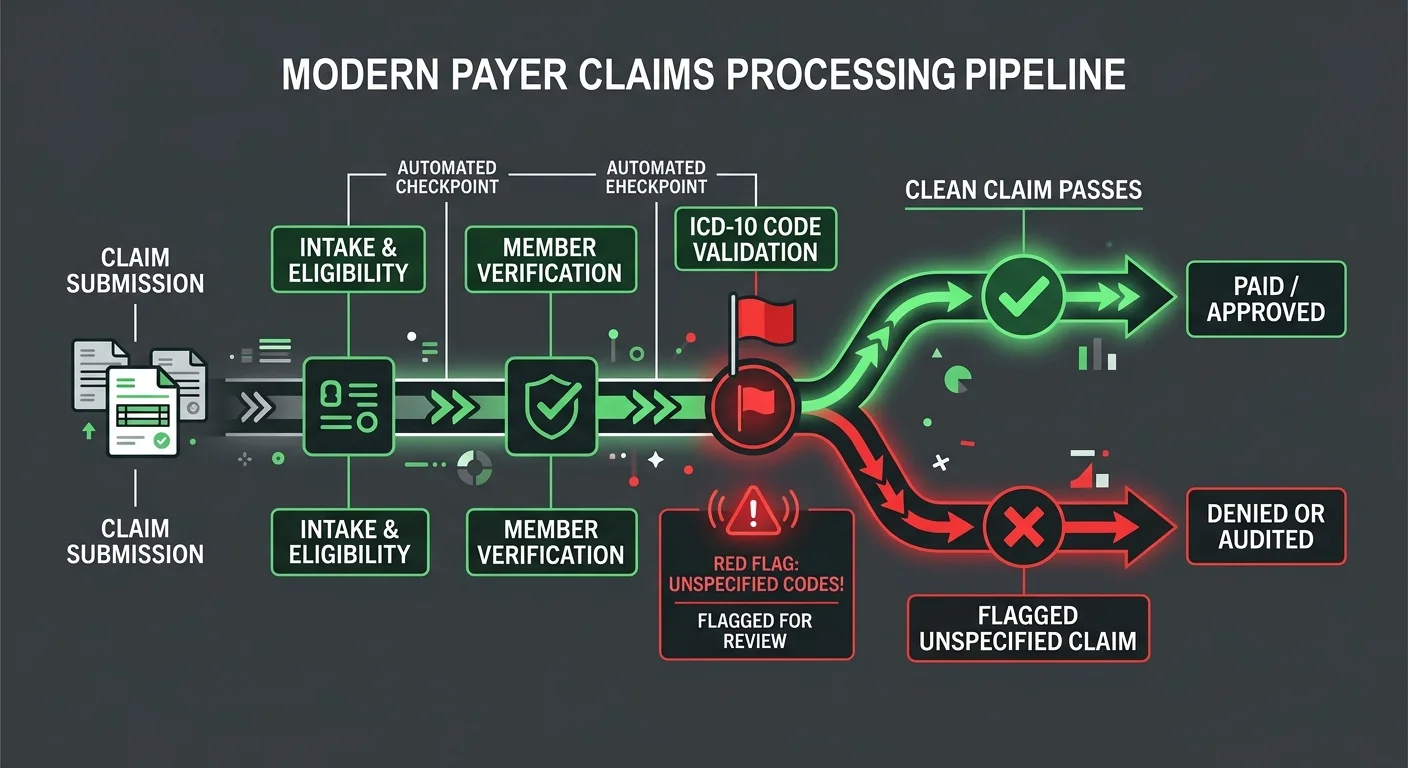
Payers aren't waiting for a reviewer to catch an unspecified code. The flag happens before the file reaches a human queue. It triggers at the automated claims editing layer — and by that point, the claim is already stopped.
CMS-configured payer systems carry a hard rule: automatically reject or flag claims that contain unspecified lateralization codes when a specific spinal region or limb is required. That isn't a reviewer's judgment call. It's logic embedded in the claims processing engine — and it runs on every submission, every cycle, without exception.
That's what catches practices off guard. The denial didn't come from a reviewer questioning the clinical picture. It came from a logic gate that identified an unspecified code in a field requiring specificity and rejected it automatically. No human judgment. No opportunity to explain.
The Specific Code Patterns That Trigger Automated Rejections
The patterns aren't obscure. They're baked into ICD-10-CM structure. For chiropractic claims, lateralization is where automated edits find them fastest.
Here's how it plays out. A spinal diagnosis code requires laterality — left, right, or bilateral. The claim submits with an unspecified value in that field. The automated edit identifies the mismatch in milliseconds. The procedure code demands a specific anatomical location. The diagnosis code doesn't deliver one. The claim flags — before a human ever opens the file.
OIG audits found that 82% of chiropractic claims reviewed didn't meet Medicare requirements — and documentation deficiencies led every category of cause. Automated edits don't catch every failure in that population. But the unspecified lateralization pattern is exactly the kind of systematic, detectable gap they're built to surface. A practice running the same EHR template default across hundreds of claims isn't just submitting one bad claim. It's producing a pattern those edits are configured to find. Practices that maintain a weekly update cadence with their billing team catch these patterns before they compound into an audit profile.
How the AT Modifier Validation Intersects With Code Specificity
The AT modifier problem doesn't start at the modifier. It starts at the diagnosis code underneath it.
CMS guidelines require the AT modifier on chiropractic Medicare claims to demonstrate active corrective treatment — not maintenance care. But that argument only holds if the underlying diagnosis is specific enough to support it. When the diagnosis code is unspecified, the AT modifier has no clinical anchor. The payer's validation logic is looking for a documentable condition that justifies active treatment. An unspecified code can't provide one. So you end up with a claim wearing the AT modifier with nothing concrete underneath it. Automated systems don't give that combination the benefit of the doubt. They flag it.
This is where practices lose the most recoverable revenue. The AT modifier was correctly applied. The service was genuinely active corrective treatment. But the diagnosis code's lack of specificity dismantled the medical necessity argument before a human reviewer ever opened the file. That's not a modifier problem. That's a documentation problem dressed up as a denial. Understanding what separates document active care from maintenance care — and demonstrating that distinction at the code level — is the only way to survive the automated edit layer with your revenue intact.
| Payer Edit Type | Trigger Condition | Claim Outcome | Revenue Impact |
|---|---|---|---|
| Lateralization specificity edit | Diagnosis code requires left, right, or bilateral designation — unspecified value submitted | Automatic rejection before human review; claim returned to provider | Immediate cash flow disruption; resubmission delay extends days in AR |
| Spinal level validation edit | Procedure code requires a defined vertebral region; claim submitted without level specificity | Claim flagged for records request or suspended pending documentation review | Revenue delayed or lost if documentation cannot retroactively support the specificity requirement |
| AT modifier clinical anchor check | AT modifier present but underlying diagnosis code is unspecified — medical necessity argument lacks a documentable condition | Modifier-level denial; active care classification challenged by payer logic | High-value active treatment revenue denied; appeals require substantial documentation reconstruction |
| Pattern frequency edit | Same unspecified code submitted repeatedly across multiple claims from the same provider — EHR template default signature detected | Audit profile triggered; practice flagged for retrospective review across claim history | Exposure extends beyond individual claims to entire billing period under review |
| Code-procedure mismatch edit | Diagnosis code category does not align with the anatomical region implied by the submitted procedure code | Claim rejected or pended; payer system identifies logical inconsistency between procedure and diagnosis | Revenue loss compounded by administrative burden of correcting both the code and supporting documentation |
What Chiropractic Practices Must Change to Eliminate Unspecified Code Risk
Knowing how the flag works means you're out of excuses. Payers reject unspecified codes before a human ever touches the file. The fix has to happen before submission — not as a damage-control response after the denial lands.
That means changing the workflow at the source. Not the clearinghouse step. The clinical documentation encounter — where the provider generates the record that every downstream billing decision depends on.
A claim with an unspecified code is a claim that asks the payer to trust you without giving them a reason to. That's not an appeals problem. It's a documentation problem — and it has to be fixed structurally, not handled on a chart-by-chart basis.
Practices that treat this as a judgment call keep producing the same pattern. Practices that embed the specificity standard into the workflow stop producing it entirely.
Clinical Documentation Standards That Support Specific Coding
Here's the baseline: the clinical record has to establish the specific spinal level, the lateralization, and the objective functional findings that support active corrective treatment. Not because it's best practice. Because without those three anchors, no specific diagnosis code is defensible — and the code selection problem has no clean answer.
The American Chiropractic Association requires practices to document quantitative measures of functional improvement to defend active care claims. That's not procedural overhead — it's the exact clinical evidence that separates a documentable, specific condition from an unspecified one.
When the record contains measurable objective data tied to a specific spinal region, the diagnosis code practically writes itself. When it doesn't, the provider is left choosing between an unspecified code and an unsupported specific one. Neither survives scrutiny.
The CDC's ICD-10-CM guidelines are direct: unspecified codes are appropriate only when clinical information is genuinely unavailable at the time of the encounter. That places the burden on documentation — not on the billing team.
When the clinical record captures specific spinal levels, lateralization, and objective findings at the time of the visit, there is no clinical justification for an unspecified code. There's only a workflow that failed to surface what the provider actually knew. Peer-reviewed analysis confirms that failure to document subluxations at specific spinal levels is a primary trigger for post-payment audits — meaning the exposure is preventable, and the practice is the one absorbing the cost of not preventing it.
How to Audit Your Own EHR Templates Before Payers Do
EHR templates don't fix themselves. The same default that produced the unspecified code last month will produce it next month — unless the template is rebuilt to enforce specificity at the point of code selection.
Start with frequency. Pull the diagnosis codes from the last 90 days of submissions and identify every unspecified code in the set.
For each one, cross-reference the corresponding clinical record. If the record contains a specific spinal level and lateralization — and most will — the template failed to surface that information at the coding step. That gap is structural, not clinical. It's fixable. Practices already running a consistent billing review rhythm have the right discipline for this audit — the same framework applies. Medicare conversion factor
Once the gaps are identified, the fix is a configuration change: replace unspecified default codes with forced-selection fields that require the provider to confirm spinal level and lateralization before the record closes.
A chiropractic RCM specialty practice — whether that expertise lives in-house or through an embedded billing partner — applies this standard as a quality gate, not a workaround. The practices that eliminate unspecified code exposure are the ones that treat the EHR template as a compliance instrument, not just a place to close the encounter.
| Documentation Element | What It Must Capture | ICD-10 Specificity It Enables | Audit Defense Value |
|---|---|---|---|
| Spinal Level Documentation | Specific vertebral segment involved (e.g., L4, C5) confirmed at the time of the encounter | Enables level-specific ICD-10-CM codes that satisfy payer anatomical requirements | Eliminates the most common automated rejection trigger — missing or unspecified vertebral level |
| Lateralization | Side of involvement documented — left, right, or bilateral — based on clinical findings, not template default | Enables laterality-specific code selection that satisfies payer edits requiring directional specificity | Closes the lateralization gap that automated claims editing systems are configured to detect and flag |
| Objective Functional Findings | Quantitative measures of functional status — range of motion, pain scales, functional outcome tools — recorded at each visit | Establishes the measurable clinical basis that distinguishes an active condition from an unspecified or maintenance-level presentation | Provides the documentable evidence base that makes a specific diagnosis code — and the AT modifier — clinically defensible |
| Active Care Justification | Documented rationale for why the current visit represents active corrective treatment, including measurable improvement trajectory | Supports the active care coding distinction required for AT modifier claims under Medicare chiropractic billing rules | Anchors the AT modifier to a specific, documented clinical condition — preventing the modifier-without-specificity flag pattern |
| EHR Template Configuration | Forced-selection fields for spinal level and lateralization that require provider confirmation before the record closes | Prevents default or placeholder codes from reaching the billing queue as the operative diagnosis | Removes the structural workflow gap responsible for systematic unspecified code patterns across high-volume claim sets |
Frequently Asked Questions
The main sections cover the mechanism. These questions cover the edges — the objections, the exceptions, and the workflow decisions that determine whether a practice fixes this or keeps producing the same exposure.
These are the questions that come up after the denial. After the audit notice. After a billing review reveals a pattern nobody caught in time. The answers are direct.
What makes unspecified diagnosis codes an automatic audit trigger in 2026?
Payer systems don't wait for a human reviewer. The flag fires at the claims editing layer — before adjudication even starts. Unspecified codes signal that clinical information was unavailable at the time of the encounter. In chiropractic, that's rarely true. The treating provider knows the spinal level. The lateralization is built into the adjustment itself. When a payer edit system encounters an unspecified code in a field that requires a specific spinal region or lateralization, it reads that gap as a documentation failure — and rejects or queues the claim. The code becomes the trigger. Not the treatment. Not the modifier. The code.
How do automated payer edits identify chiropractic claims with unspecified codes?
The edit validates lateralization and spinal level fields against the submitted diagnosis code. When an unspecified code appears where a specific one is required, the edit fires. It's not a judgment call. There's no clinical context being weighed. The code either satisfies the field requirement or it doesn't — and an unspecified code doesn't. Here's what makes this dangerous at scale: a single unspecified code is a missed claim. A pattern of them — exactly what template-defaulted workflows produce — is an audit profile. The automated edit doesn't distinguish between a one-time error and a systemic habit. It just keeps finding the same gap.
What specific clinical scenarios allow for unspecified coding without triggering a denial?
The standard is narrow. Unspecified codes are appropriate only when clinical information is genuinely unavailable or non-specific at the time of the encounter. In chiropractic, that threshold is uncommon. A new patient presenting with diffuse, unlocalized symptoms and no completed examination may meet it. A returning patient with a documented adjustment at a specific spinal level does not. If the record contains the level and the lateralization — and in most chiropractic encounters it does — the code has to reflect it. There's no exception for an EHR template that defaulted to unspecified. There's no carve-out for a provider who assumed the extra detail wasn't required.
How does using an unspecified ICD-10 code impact the AT modifier validation?
It pulls the clinical anchor out from under the AT modifier. The AT modifier tells Medicare the service was active corrective treatment — not maintenance care. But that argument only holds when the underlying diagnosis supports it with specificity. CMS validation logic looks for a documentable condition when it processes an AT modifier claim. An unspecified code can't provide one. So the modifier was correctly applied. The treatment was genuinely active. And the claim still fails — because the diagnosis code couldn't anchor the medical necessity argument. The treatment wasn't the problem. The documentation was. That's the kind of loss that's nearly impossible to recover from after the fact.
What steps can chiropractic practices take to audit their own EHR templates for unspecified codes?
Pull the diagnosis codes from the last 90 days of submissions. Identify every unspecified code in that set. For each one, go back to the clinical record. If the record documents a specific spinal level and lateralization — and most will — the template failed to surface that information at the coding step. That gap is structural. It's also fixable. The American Chiropractic Association requires quantitative measures of functional improvement to defend active care claims. If those measures exist in the record but the template still defaults to an unspecified code, the template is the problem. Replace the unspecified defaults with forced-selection fields that require spinal level and lateralization confirmation before the record closes. The clinical information is already there. The workflow just isn't capturing it.
Coding Specificity Is Not Optional in 2026
The automated edit layer doesn't care how good the clinical encounter was.
It doesn't know the provider identified the exact spinal level. It doesn't know the treatment was genuinely active and corrective. It sees an unspecified code in a field that required specificity — and the claim stops.
That's not a paperwork technicality. That's a structural invitation for scrutiny that payer systems are built to accept every single time.
This isn't something the billing team fixes after the fact. The fix belongs at the point of documentation — where the clinical record is built, not where it gets submitted.
Practices that embed specificity requirements into their EHR templates stop producing unspecified codes. Practices that leave the templates unchanged keep producing the same pattern — claim after claim, building an audit profile one submission at a time.
The CDC's ICD-10-CM guidelines are clear: unspecified codes are appropriate only when the clinical information is genuinely unavailable. In chiropractic, that threshold is rarely met. Every claim that uses an unspecified code when specific information exists is a claim that failed its own documentation — and a claim that asks the payer to trust you without giving them a reason to.
The practices that survive 2026 payer scrutiny aren't the ones that submit faster. They're the ones that stopped trusting their EHR template to do the clinical thinking.
That requires a billing partner whose expertise runs deep enough to catch the pattern before it becomes a profile — one who reviews the diagnosis against the documentation before submission, and who tells you what they find without waiting to be asked. That's the standard Bushido Billing was built to hold.
Faster submission doesn't close the trust gap. A human-validated coding model does. If your current workflow is still producing unspecified codes, the audit profile is already building — and the only question left is whether you find it before the payer does.
An unspecified code doesn't just slow down a claim. It hands the payer a reason to audit everything behind it. The exposure is already in your submissions — the only question is whether you find it first or they do.

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet