

How to Defend Your Practice Against the 2026 ICD-10 SDOH and Medicare Regulatory Updates?
The 2026 regulatory updates are not an EHR problem. They are a clinical judgment problem.
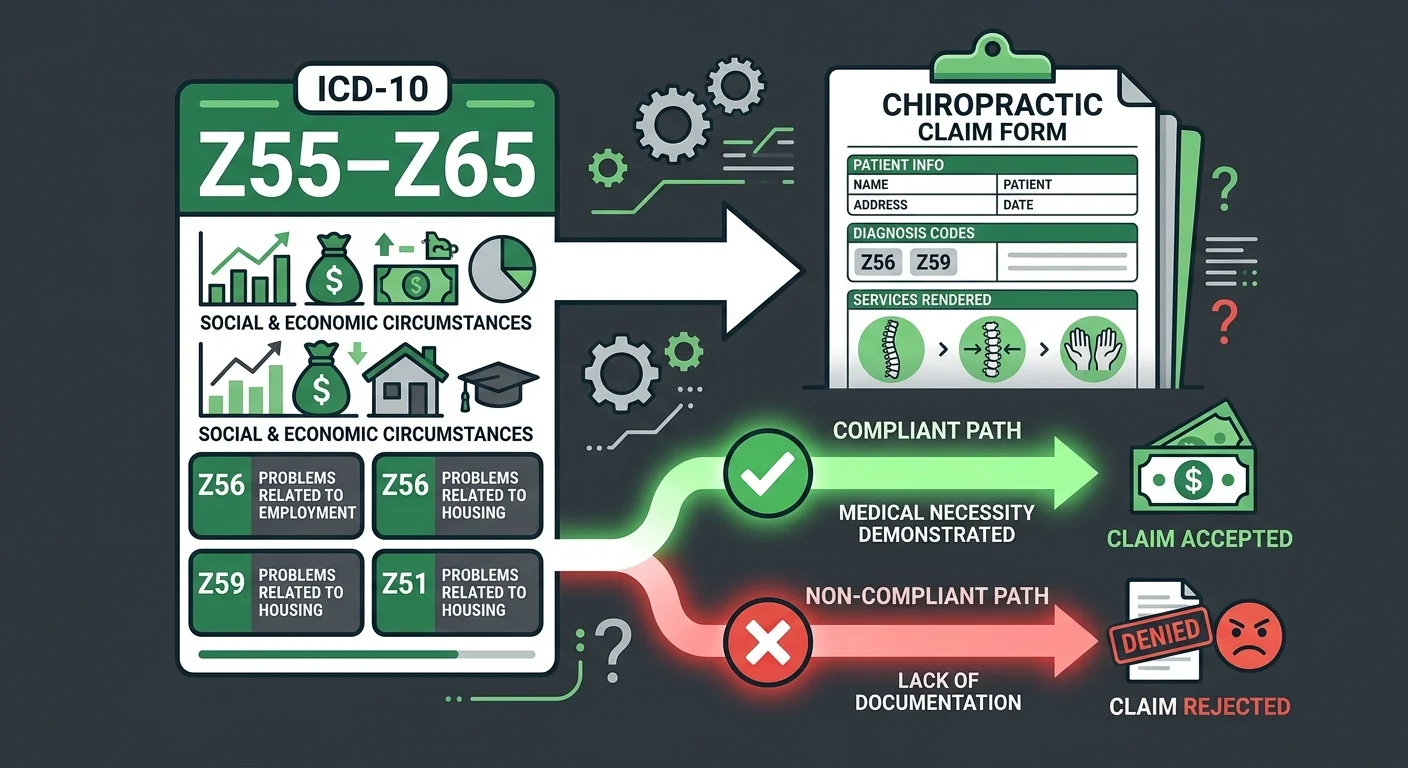
CMS has expanded its push for structured Social Determinants of Health (SDOH) documentation. Providers must now apply ICD-10-CM codes in the Z55–Z65 range to capture factors like housing instability, food insecurity, and transportation barriers. These are not optional fields. They are tied directly to payer scrutiny and documentation completeness — and they determine whether a claim pays or denies.
Medicare's AT modifier remains a persistent denial trigger. It must be appended to CPT codes 98940, 98941, or 98942 to signal that care is active and medically necessary — not maintenance. Getting that boundary wrong produces automated denials. They compound fast.
Neither of these requirements is new in concept. Both are failing in execution.
ICD-10-CM coding guidelines are revised annually, effective each October 1st. That cadence demands ongoing vigilance — not a one-time configuration update. Structured SDOH coding has one of the lowest adoption rates in clinical documentation: research shows fewer than 2.5% of social needs are captured using structured Z-codes, even when those needs appear in progress notes.
The gap between knowing a requirement exists and executing it correctly on every claim is where practices lose revenue. Automation has no pathway once a claim requires a medical necessity argument. That gap is closed by a billing partner who understands chiropractic-specific documentation standards, tracks regulatory changes as they happen, and treats modifier mapping and SDOH coding as clinical revenue imperatives.
That is the standard Bushido Billing holds its billing operations to. It is the standard any chiropractic practice should demand from whoever is managing their claims in 2026.
Last Updated: June 22, 2026
- • What the 2026 ICD-10 and Medicare Regulatory Changes Actually Mean for Chiropractic
- • What the 2026 Changes Demand From Your Billing Process
- • Why EHR Software Cannot Protect You From 2026 Regulatory Risk
- • What Strong 2026 Compliance Billing Looks Like
- • What This Level of Documentation Discipline Requires
-
• Frequently Asked Questions
- • How do the 2026 Social Determinants of Health (SDOH) codes impact chiropractic clinical documentation?
- • What is the correct way to map AT modifiers on Medicare claims to prevent automated denials in 2026?
- • Why can't our clinic's EHR software handle the new 2026 Medicare coding updates automatically?
- • Will adding SDOH Z-codes to chiropractic billing increase the risk of an audit?
- • What are the common points of failure when chiropractic staff attempt in-house billing for SDOH codes?
- • The Only Regulatory Defense That Actually Holds
What the 2026 ICD-10 and Medicare Regulatory Changes Actually Mean for Chiropractic
These are not temporary adjustments. The 2026 Medicare documentation requirements are a permanent raise in the floor. Practices waiting to see how things settle are already behind the standard Medicare is adjudicating against right now.
Two requirements are hitting at once. CMS has expanded structured SDOH data collection — providers are now expected to apply ICD-10-CM codes in the Z55–Z65 range to document social factors that affect patient outcomes. And the code set itself changes every year. CDC guidelines set annual revisions effective each October 1st. That means the codes your billing operation trained on last year are not the codes Medicare is reading today.
Most practices know something changed. What they're missing is what correct application actually demands on every claim, every visit. This is not an admin task you delegate to an intake form. It requires clinical judgment — and clinical judgment does not run on autopilot.
The SDOH Z-Code Expansion and Why Chiropractors Cannot Ignore It
The SDOH Z-code expansion is not a paperwork formality — CMS is using structured Z-code data to evaluate care coordination and flag documentation gaps across Medicare claims. A practice that writes social needs into progress notes but never maps them to structured codes is invisible to that system. And invisible, in this context, means payer scrutiny and delayed reimbursement.
The five SDOH domains each carry corresponding Z-code ranges. Mapping a patient's barrier to the correct code in the Z55–Z65 range is not an EHR dropdown decision. You need to understand what each domain signals to a payer — and that understanding does not come from software. It comes from someone who reviews that claim against the clinical picture.
And NIH research confirms what practices are already experiencing — social needs get written into progress notes, but almost never captured in the structured codes payers actually read. Less than 2.5% of documented social needs end up in structured Z-codes. That is not a documentation style preference. That is a billing failure with direct revenue consequences. Practices that want to know exactly which codes apply to their patient population should start with 2026 SDOH codes apply.
Why High-Volume Billing Struggles With the New Documentation Load
Volume-first billing is optimized for speed. Clean claims move fast. Complex documentation reviews do not. That asymmetry is not a quirk — it is the structural reason high-value claims get abandoned.
When a claim requires SDOH Z-code mapping alongside AT modifier verification, the volume model has no efficient pathway for that review. It gets deprioritized. Then it ages. The full-service chiropractic billing model is built differently — a dedicated biller reviews each claim against chiropractic-specific documentation standards, not against a queue optimized for submission speed.
ICD-10-CM updates land every October 1st. A volume-first operation absorbs that at the system level — updated crosswalks, maybe a staff memo, then back to the queue. Careful billing absorbs it at the claim level. Active documentation gets audited against the current standard. Modifier mismatches get caught before they become denials. That is not the same service. In 2026, that difference shows up in recoverable revenue.
| Regulatory Change | Effective Date | Primary Impact on Chiropractic Billing | Documentation Action Required |
|---|---|---|---|
| SDOH Z-Code Expansion (ICD-10-CM Z55–Z65) | Effective October 1, 2025 (FY2026) | CMS now expects structured Z-code documentation alongside clinical codes — not just narrative notes. Claims missing structured SDOH coding face increasing payer scrutiny and documentation gaps during audits. | Identify which of the 5 SDOH domains apply to each patient. Map social barriers to the correct Z-code range. Convert progress note language into structured, payer-readable codes on every applicable claim. |
| Annual ICD-10-CM Code Set Revision | October 1st of each fiscal year | Code specificity requirements shift annually. A billing operation using last year's crosswalks is adjudicating against an outdated standard — creating silent denial risk on claims that appear correct at the time of submission. | Audit active coding documentation against the current fiscal year's ICD-10-CM guidelines. Update modifier mapping and code-to-condition logic before the October 1st effective date — not after denials surface. |
| AT Modifier Verification (CPT 98940, 98941, 98942) | Ongoing — heightened scrutiny under 2026 Medicare adjudication | Medicare automated systems flag claims where active treatment versus maintenance care documentation is ambiguous or missing. The AT modifier must be defensible at the clinical documentation level — not just appended by habit. | Review patient records for clear medical necessity documentation before each claim submission. Ensure the clinical record supports active care status. Treat the AT modifier as a clinical declaration, not a billing checkbox. |
| SDOH Domain-to-Code Mapping (5 Federal Domains) | Aligned with Healthy People 2030 and CMS structured data initiative | Each of the 5 SDOH domains — economic stability, education access, healthcare access, neighborhood and built environment, and social and community context — carries distinct Z-code ranges. Incorrect domain assignment produces miscoded claims that don't reflect the patient's documented social barriers. | Train billing staff to recognize which patient circumstances map to which SDOH domain. Establish a documentation protocol that converts clinical observations into the correct Z-code range before claim submission — not after a payer rejection. |
| Care Coordination Documentation Expectations | Tied to CMS SDOH data collection expansion (FY2026 forward) | Payers are using structured SDOH data to evaluate care coordination patterns across Medicare claims. Practices documenting social needs only in unstructured notes are invisible to this system — and increasingly vulnerable to documentation-based coverage disputes. | Establish a clinical documentation workflow that routes relevant social needs observations into structured Z-code fields. Treat SDOH coding as a revenue protection measure, not an optional clinical data point. |
What the 2026 Changes Demand From Your Billing Process
Volume-first billing isn't incompetence. It's a rational model built around one goal: move clean claims fast.
That works — until the regulatory environment introduces the kind of complexity that breaks the clean-claim assumption.
The 2026 updates break it.
AT modifier mapping is a clinical judgment call on every single Medicare visit. SDOH Z-code documentation requires someone who understands what each code signals to a payer — not a processor working a submission queue.
Those are not the same skill set. And a volume model does not budget for either one.
That's the structural mismatch. Volume models aren't designed to slow down for complex claims.
When a model isn't built for something, it doesn't do it. Doesn't matter how competent the people running it are.
The Submission-Speed Trap: What Volume Models Actually Optimize For
Here's what volume models actually measure: submission speed and claim count.
Not denial rate on complex visits. Not recovery rate on high-friction Medicare claims.
Submission speed.
That metric works fine on a straightforward claim. Clean diagnosis, standard CPT code, no modifier ambiguity — it moves fast, and the volume model performs exactly as designed.
But the AT modifier on CPT codes 98940, 98941, or 98942 is not a simple claim event. It's a documentation decision. Someone has to confirm that care is active and medically necessary — not maintenance — on every single Medicare visit.
ACA Medicare guidelines are precise on that boundary. So are the automated denial systems that fire when it's wrong.
Each of those requirements is a judgment call. Volume models don't budget time for that review.
So it gets skipped. Or worse — it gets assumed. The biller moves to the next claim in the queue, and the documentation gap stays open.
Visit management has gotten more complex, not less. Practices handling these layers in-house or through a throughput-first operation are carrying that risk on every qualifying visit — including those that involve the g2211 add-on code.
High-Complexity Claims Are the First Casualty of a Volume Model
When a claim requires SDOH Z-code mapping, AT modifier verification, and documentation that defends medical necessity — the volume model deprioritizes it.
Not because someone decided to. Because the model has no efficient pathway for that level of review.
So the claim waits.
It ages. In many cases, it dies. The practice never sees that revenue — because no one flagged it, no one appealed it, and no one told the provider it was gone.
NIH research puts a number on the pattern: less than 2.5% of social needs are captured using structured ICD-10-CM Z-codes, even when those needs are written directly into clinical notes.
The volume model isn't closing that gap. It's perpetuating it — one unworked claim at a time.
The 2026 updates don't break volume-first billing because they're technically hard. They break it because they require the one thing a throughput model can't budget for: time spent defending a single claim.
That's where practice revenue disappears.
Automation has no pathway once a claim needs a medical necessity argument. That gap gets closed by a billing partner who treats complex claims as the work — not as the exception.
| Billing Model Type | Claim Submission Speed | Complex Denial Defense | SDOH Z-Code Documentation | AT Modifier Audit Defense | Revenue Recovery on Hard Claims |
|---|---|---|---|---|---|
| Volume-First / Generalist Billing | Optimized — claims submitted at maximum throughput speed | Minimal — complex denials are deprioritized when appeal cost exceeds throughput budget | Inconsistent — social needs captured in notes but rarely converted to structured Z-codes | Assumed — modifier application is not audited per visit; errors surface only after denial | Low — high-friction claims age and die without dedicated follow-up |
| EHR Platform as Billing Solution | Fast submission — the EHR is designed for claim output, not claim defense | None — EHR software has no appeal or medical necessity argument pathway | Dropdown-dependent — structured code mapping requires clinical judgment the software cannot apply | Not performed — modifier logic is rule-based; active vs. maintenance distinction requires human review | Not applicable — revenue recovery requires human intervention the platform does not provide |
| Generalist Billing Company | Moderate — processing speed varies; chiropractic-specific complexity slows review | Limited — generalists lack the specialty knowledge to defend chiropractic medical necessity arguments | Ad hoc — SDOH Z-code specificity for chiropractic patient populations is not a core competency | Inconsistent — AT modifier rules require chiropractic-specific documentation knowledge generalists may not apply correctly | Variable — recovery depends on whether the biller recognizes the claim is worth defending |
| Chiropractic-Focused Specialist Billing | Deliberate — submission speed is balanced against documentation accuracy on every claim | Proactive — multi-step appeals and medical necessity arguments are a core service function, not an exception | Structured — dedicated billers map social factors to the correct Z-code range with clinical documentation context | Per-visit — each Medicare claim is audited for active vs. maintenance care boundary before submission | High — hard claims are flagged, worked, and defended rather than aged and abandoned |
Why EHR Software Cannot Protect You From 2026 Regulatory Risk
Here is the assumption that costs practices the most: the EHR handles billing.
It does not. It handles submission. Those are not the same thing.
EHR platforms are built to move claims out the door. Not to defend them when they come back wrong.
Denial management, modifier auditing, SDOH documentation review — none of that is automated. All of it requires human judgment. And in 2026, those are the exact skills Medicare is testing on every qualifying claim.
ICD-10-CM codes are revised annually. Every October 1st, the set changes. That means the coding logic your EHR was configured with at the start of the year is not the logic Medicare is adjudicating against by the end of it.
No automatic software update closes that gap at the claim level. Someone has to review it, catch the mismatch, and act before the denial lands. The platform will not do that. It cannot.
What EHR Platforms Actually Do — and Where They Stop
EHR platforms do what they were built to do. Capture clinical data, generate a claim, push it to the clearinghouse. For a clean visit — standard diagnosis, standard CPT, no modifier complexity — that workflow holds.
But the moment documentation complexity enters the picture, the EHR has no pathway. An AT modifier decision. A contested medical necessity boundary. A social factor that belongs in the Z55–Z65 range. The platform does not pause to review any of it. It moves to the next claim.
The platform is not broken. It is doing exactly what it was designed to do.
The problem is when practices treat the software's output as a complete billing operation. It is not. The EHR ends exactly where the actual work begins.
Whether a visit qualifies as active and medically necessary versus maintenance is a clinical documentation call. It has to be made before the claim goes out — not flagged after it comes back denied.
An EHR can populate the modifier field. It cannot evaluate the documentation behind it. That evaluation is where denials are prevented or created. It requires someone who understands AT modifier mapping — and acts on it before submission, not after.
The Structured Z-Code Gap: Why Social Needs Stay in Progress Notes
CMS has told providers to use structured ICD-10-CM codes in the Z55–Z65 range. Housing instability, food insecurity, transportation barriers — document them with the right code, not a progress note.
The directive is clear. The compliance rate is not.
Research on clinical EHR repositories found that while social needs are regularly documented in progress notes, less than 2.5% are captured as structured ICD-10-CM Z-codes.
That is not a clinician failure. EHR systems do not prompt for Z-code specificity at the point of care. And billing operations running on throughput do not audit for it afterward. The gap is not an oversight — it is baked into both systems.
So the social need gets noted. The structured code never gets applied. The payer never sees it in a format they can read.
Then the practice gets scrutiny on documentation that should have protected it. The gap is not in the clinical encounter — it is in the documentation decision that should have followed. No EHR makes that call. No volume-first billing operation audits for it. Practices that want to know which new ICD-10 SDOH codes for chiropractors apply to their patient population have to start by closing that gap deliberately.
| Task | EHR Platform Capability | Human Billing Specialist Capability | Revenue Risk if Left to Automation Alone |
|---|---|---|---|
| AT modifier determination (active care vs. maintenance) | Flags the modifier field on CPT codes 98940, 98941, 98942 — does not evaluate the documentation behind the decision | Reviews visit documentation against Medicare's active medical necessity standard before claim submission; catches ambiguous boundaries before they trigger a denial | Claims submitted without confirmed medical necessity documentation face automated denial with no recovery pathway at the claim level |
| SDOH Z-code mapping to the Z55–Z65 range | May include Z-code fields in the template; does not audit whether the correct code was applied or prompt for specificity at the clinical moment | Identifies which social determinant domain applies to the patient encounter and maps it to the correct structured code payers can read and adjudicate | Social needs documented only in progress notes are invisible to payers — the structured code is the only format that counts toward care coordination credibility |
| Annual ICD-10-CM code update absorption (effective October 1st each year) | Receives system-level crosswalk updates; does not audit active claims against new code specificity requirements at the individual visit level | Reviews documentation standards against the updated code set, identifies specificity gaps in active claims, and adjusts billing logic before denials accumulate | Claims adjudicated under the updated code set without a claim-level review will produce denials that look like coding errors but reflect an unaudited transition |
| Denial review and medical necessity appeals | Routes denied claims to a worklist; does not construct a medical necessity argument, review the clinical file, or draft an appeal | Analyzes the denial reason, pulls supporting documentation, constructs the clinical argument, and submits a multi-step appeal with payer-specific language | Denied claims that are not actively appealed with clinical documentation age out of the recovery window — the revenue is permanently lost |
| Documentation audit prior to claim submission | Validates that required fields are populated; does not evaluate whether the documentation meets payer medical necessity or modifier standards | Reviews the clinical record against billing requirements before submission, catching modifier mismatches and documentation gaps that would trigger automated denials | Claims submitted on incomplete or ambiguous documentation create denial patterns that compound over time — each cycle harder and more expensive to reverse |
What Strong 2026 Compliance Billing Looks Like
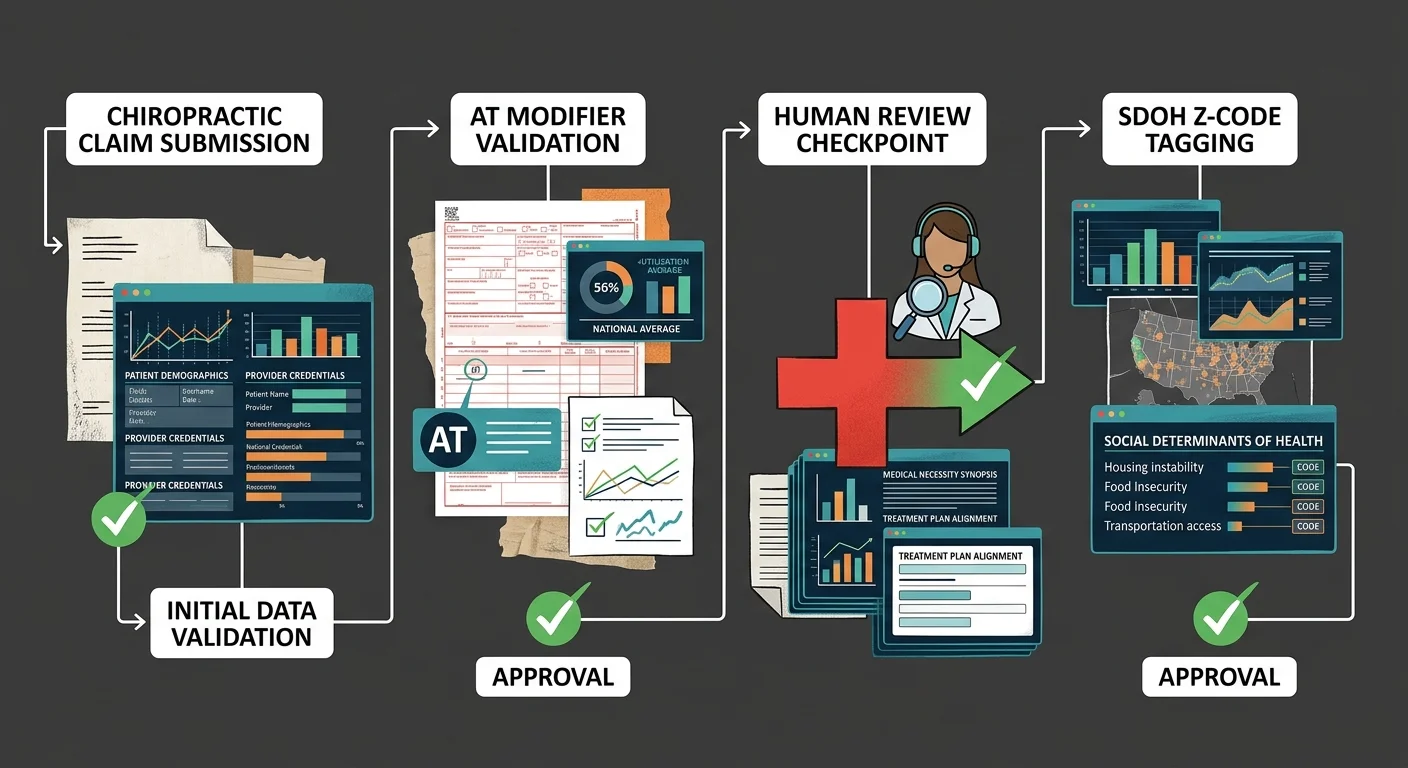
Done well, regulatory updates aren't absorbed at the system level. They're absorbed at the claim level.
That means auditing modifier decisions before claims go out. Reviewing documentation against current standards — not last year's configuration. Catching the mismatch before it triggers a denial.
That is a fundamentally different service. Not a faster version of the same thing.
The 2026 updates come down to two things automation cannot do. First: make a clinical judgment call on AT modifier decisions. Second: apply structured SDOH documentation in a format payers actually process.
Neither of those gets solved by a clearinghouse queue built for throughput. Both require a human who knows chiropractic-specific documentation standards — and who is accountable when a claim comes back wrong.
That accountability is the core of human intelligence and automated coding.
Dedicated biller assignment is not a customer service feature. It is the architecture that makes claim-level review possible.
One person who knows your patient mix, your documentation patterns, and your payer requirements. That is how modifier errors get caught before submission — not discovered at audit.
In a regulatory environment where a single AT modifier error on a Medicare claim fires an automated denial, that architecture is what protects revenue.
AT Modifier Mapping: The Human Judgment Layer Automation Cannot Replace
The AT modifier is not a checkbox. It is a clinical determination.
Under Medicare rules, the AT modifier must be appended to CPT codes 98940, 98941, or 98942 to indicate that care is active, medically necessary, and distinct from non-covered maintenance care.
That determination must be made correctly on every single qualifying visit. There is no rounding up. There is no approximate.
A volume-first operation cannot consistently make that determination. The model does not budget time for the documentation review the judgment requires.
Claim-level billing does. Because it's built around reviewing each claim — not submission-level throughput. The biller working your Medicare claims understands the active-care boundary. They know what the documentation needs to say. And they flag the visit before it goes out wrong.
That is not a speed advantage. That is a structural one.
That is why weekly updates on claim status matter structurally — not as a communication courtesy, but as the operational cadence that surfaces AT modifier issues before they age into denials.
When a practice knows what is happening with its Medicare claims every week, documentation errors can be corrected while the clinical encounter is still recent. When it does not, the practice finds out at audit.
Those are not equivalent outcomes.
SDOH Documentation as a Revenue Defense Strategy, Not a Checkbox
CMS has directed providers to apply ICD-10-CM codes Z55–Z65 — housing instability, food insecurity, transportation barriers. These are not optional fields. They are documented federal expectations.
HHS stated it plainly: structured SDOH data collection is central to the national strategy for reducing health disparities. The expectation is in writing.
The execution is not happening. And that is not a clinical failure. It is a billing failure.
Done right, SDOH Z-code documentation is a revenue defense decision. Not administrative overhead.
That means auditing whether a documented social barrier has a corresponding structured code in the Z55–Z65 range — not just a note in the progress record.
Payers read structured codes. They do not read unstructured notes. If the code is not there, the documentation is not there.
The practices that hold their footing after the 2026 updates are not the ones with the fastest submission pipeline. They are the ones whose billing partner treats every complex Medicare visit as a documentation event — not just a claim to push through.
That means auditing AT modifier decisions before claims go out. Mapping Z-codes to the correct range. Knowing what each code signals to a payer — and being ready to defend medical necessity when a claim comes back challenged.
That is the operational difference between a high-volume model and claim-level specialty billing. And it is the difference that shows up in recoverable revenue.
| Compliance Action | Who Performs It | Frequency | What Happens Without It |
|---|---|---|---|
| AT modifier review on Medicare visits | Dedicated specialty biller with chiropractic-specific documentation knowledge | Every qualifying claim before submission | Modifier applied incorrectly or omitted — automated denial issued; revenue lost without appeal pathway |
| SDOH Z-code documentation audit | Specialist biller reviewing structured vs. unstructured clinical notes | Ongoing — aligned to each annual ICD-10-CM update cycle | Social needs captured in progress notes only — payer never reads them; structured documentation gap widens |
| Active vs. maintenance care boundary determination | Human reviewer trained in chiropractic Medicare documentation standards | Per visit — prior to claim submission | Maintenance care billed as active treatment — audit exposure created; non-covered care paid initially, then recouped |
| Annual ICD-10-CM update integration | Specialist biller absorbing regulatory changes at the claim level | Each October 1st effective date — applied to active claim workflow | Outdated code logic remains in submission pipeline; claims adjudicated against current codes, denied on specificity |
| Weekly claim status communication | Dedicated biller reporting directly to the practice | Weekly — surfaces modifier and documentation issues while clinical encounters are still recent | Documentation errors age undetected; practice discovers billing failures at audit rather than at correction |
| Denial appeal for complex Medicare claims | Human specialist with medical necessity argument capability | As needed — triggered by payer rejection requiring clinical documentation review | Complex denials deprioritized or abandoned; recoverable revenue permanently written off |
What This Level of Documentation Discipline Requires
Not every practice is ready for this.
That's not a judgment — it's a qualification. Closing the gap between EHR submission and actual revenue recovery requires something from your side of the table too.
Documentation discipline at this level is an ongoing process. You don't set it up once and walk away.
Practices that get the most out of it come in knowing that. The ones that don't find out fast.
So read the qualification gate below carefully.
The behaviors on both sides of it matter more than any feature list.
The Practice Behaviors That Make This Partnership Work
The practices this model works for aren't hard to spot. They give EHR access without making it a negotiation. They turn documentation requests around fast.
That speed isn't administrative housekeeping. An AT modifier decision on CPT codes 98940, 98941, or 98942 has to be evaluated before the claim goes out — not after the denial lands. That window is narrow. Miss it, and you're not looking at a correction. You're looking at an unworked denial aging past the point of return.
They also engage with the numbers. When a billing partner surfaces a pattern — a recurring modifier error, a cluster of Z-code documentation gaps — the practice responds.
That feedback loop is how problems get corrected at the visit level instead of the audit level. A practice that engages with its billing data weekly can adapt in real time. A practice that doesn't absorbs the loss instead.
In 2026, that distinction has a dollar value attached to it — tied directly to the fee schedule and conversion factor shifts.
Here's the structural reality: less than 2.5% of social needs get captured using structured ICD-10-CM Z-codes — even when those needs are clearly written into clinical notes.
Closing that gap requires a practice willing to treat documentation decisions as revenue decisions. And a billing partner willing to audit for them.
Both halves have to show up. One without the other doesn't close the gap.
When Bushido Billing Is Not the Right Call
If your first question is the rate, this isn't the right call.
Rate tells you the cost. It tells you nothing about how much revenue your practice actually recovers. Those are different numbers. And if the conversation starts with the first one, it can't get to the second.
If your practice won't cooperate with EHR access, respond to documentation requests, or engage with weekly claim status updates — this model won't perform for you.
Billing doesn't run independently of the provider. The AT modifier decision on a Medicare visit requires clinical documentation that only your practice can produce. If that documentation isn't available when the biller needs it, the claim goes out wrong.
There's no workaround for that.
And if your practice runs primarily on cash pay with minimal insurance complexity, Bushido Billing isn't your right partner.
The expertise here is deep and specific — chiropractic and allied health insurance billing, Medicare modifier compliance, SDOH Z-code documentation, denial management, and appeals. That depth is the point.
Vertical specialization is a feature, not a limitation. We don't serve every practice type because depth requires focus.
Frequently Asked Questions
But conviction doesn't close the gap. Specific answers do.
Skeptical practice owners don't move on arguments. They move on clarity — the kind that tells them exactly what changes, what breaks, and what it costs if they get it wrong.
These are the five questions chiropractic practices ask when they finally sit down with what the 2026 updates actually demand. The answers here are honest — not optimistic.
How do the 2026 Social Determinants of Health (SDOH) codes impact chiropractic clinical documentation?
The impact lands at the documentation level. And it's not subtle.
CMS has directed providers to apply ICD-10-CM codes in the Z55–Z65 range to capture structured data on social factors shaping patient health — housing instability, food insecurity, transportation barriers. For chiropractic practices, that means the clinical encounter can't stop at the musculoskeletal complaint. If a documented social barrier is affecting a patient's recovery, it needs a structured code a payer can read. A progress note doesn't count.
Payers use structured codes to evaluate claims and flag inconsistencies. A practice that writes social needs into clinical records but never maps them to the Z55–Z65 range is handing a payer an inconsistency they can use against you. That's not a documentation style preference. It's a revenue defense failure — and in 2026, closing that gap isn't optional.
What is the correct way to map AT modifiers on Medicare claims to prevent automated denials in 2026?
The AT modifier maps correctly when your documentation draws a hard line between active, medically necessary care and non-covered maintenance. Under Medicare rules, it must be appended to CPT codes 98940, 98941, or 98942 — and that distinction has to hold up if a payer pulls the claim. It's not a checkbox. It's a clinical judgment call made before submission.
Here's where most practices get hurt. They're reviewing AT modifier decisions after the denial fires. That's backwards. The determination happens before the claim goes out — against the actual documentation from that specific visit, not a blanket policy.
Claim-level review catches that gap before submission. High-volume throughput billing can't. The per-claim review time isn't in the model. Clean claims move fast. Complex modifier decisions get batched and pushed through without the individual review Medicare requires. That's the claim that comes back denied — and by then, the appeal window is already shrinking.
Why can't our clinic's EHR software handle the new 2026 Medicare coding updates automatically?
Your EHR is a claim submission tool. That's what it was built for. What it can't do is evaluate clinical judgment — and the 2026 updates require clinical judgment at the coding level.
The ICD-10-CM guidelines are revised annually, effective October 1st. The 2026 cycle includes expanded SDOH code specificity. Your EHR can add new codes to a dropdown. It cannot determine which Z-code accurately maps to a patient's documented social barrier. It cannot evaluate whether your AT modifier decision is clinically defensible. It cannot flag a documentation gap before it becomes a denial.
The research confirms what practices are already running into: less than 2.5% of social needs are captured using structured ICD-10-CM Z-codes, even when those needs are clearly documented in clinical records. The technology is there. The human judgment layer isn't — and no software update adds it.
Will adding SDOH Z-codes to chiropractic billing increase the risk of an audit?
Adding structured Z-codes doesn't increase audit risk. Missing them when your documentation already supports them does.
Payers are looking at whether structured SDOH data lines up with what you're documenting clinically. A practice that records social barriers in progress notes but never maps them to the Z55–Z65 range creates an internal inconsistency. That inconsistency is harder to defend than consistent, structured coding — because it looks like selective documentation, not oversight.
The real audit exposure in 2026 sits with AT modifier decisions on Medicare claims for CPT codes 98940, 98941, or 98942 where the documentation doesn't clearly support active, medically necessary care. A practice with clean, structured coding that maps Z-codes to clinical findings is in a stronger audit position — not a weaker one. Structured codes are evidence of documentation discipline. That's an asset, not a target.
What are the common points of failure when chiropractic staff attempt in-house billing for SDOH codes?
There are three failure points. They compound.
The first is recognition. Staff attempting in-house SDOH coding often don't know which patient interactions warrant a Z-code — or which specific code in the Z55–Z65 range maps to a documented social barrier. ICD-10-CM guidelines update annually with revisions effective October 1st. Specialty-specific application of those updates requires continuous training that general clinical staff aren't resourced to maintain.
The second is structured capture. Research shows that less than 2.5% of documented social needs end up in structured ICD-10-CM Z-codes — the rest stay buried in unstructured progress notes. In-house staff default to the documentation format they know. The structured code never gets applied.
The third is the AT modifier boundary. Staff without chiropractic-specific Medicare billing expertise can't reliably evaluate whether a visit on CPT codes 98940, 98941, or 98942 meets the active-care standard. They won't always recognize when the documentation is insufficient. So the claim goes out wrong — and comes back as a denial no one is positioned to appeal.
The Only Regulatory Defense That Actually Holds
The 2026 updates are not a software problem. They never were.
But the billing industry's default response to clinical judgment problems is to route them through a clearinghouse queue and call it covered. That's not a defense. That's a delay with a due date — and the payer knows it.
Automation has no pathway once a claim requires a medical necessity argument. That's not a criticism — it's a design fact.
An EHR submits claims. It does not defend them. A volume-first operation processes clean claims at scale. It does not evaluate whether the AT modifier on a Medicare visit is clinically supported. It does not audit whether a patient's documented social barrier maps to a structured Z-code the payer will actually read.
Those decisions require a human who understands chiropractic-specific documentation standards — and has the time budgeted to make them correctly. That's the model Bushido Billing is built around: dedicated biller assignment, claim-level review, and weekly communication that surfaces problems before they become denials.
The regulatory environment hasn't adjusted. It has changed.
Practices that hold their ground after 2026 are the ones that stopped treating billing as a background function. They treat it as a disciplined operation — specialty expertise, human accountability, claim-level review. That's the only position that holds when a payer challenges an AT modifier decision, flags a documentation gap, or rejects an SDOH code that never made it out of a progress note.
Automation submits claims. Human judgment defends them. In 2026, the gap between those two things is the gap between recoverable revenue and written-off loss — and the practices still running volume-first operations are about to find out which side of that line they're on.
That gap doesn't close on its own. The AT modifier decisions your staff is making right now, the SDOH documentation sitting in unstructured notes, the denials building in your AR — those aren't software problems. They're judgment calls that automation can't make. Bushido Billing works with chiropractic practices that are done guessing where the revenue is going. Book a Call to see exactly where your billing operation is exposed.
Book a Call to see where your billing stands before October hits

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet