

How to Conduct an Internal Coding Audit Before the 2026 Regulatory Changes Take Effect?
An internal coding audit is a systematic review of clinical documentation, modifier usage, and diagnostic coding accuracy — conducted before a payer or federal auditor initiates one.
The audit covers four areas: whether documentation supports the medical necessity standard for each claim, whether CPT codes 98940, 98941, and 98942 are applied correctly to covered manual spinal manipulation services, whether the active treatment modifier is consistently documented, and whether diagnostic codes reflect the annual ICD-10 updates CMS mandates every October 1.
The numbers behind this are hard to ignore. OIG audit history shows documentation error rates exceeding 80% in targeted modifier reviews. Peer-reviewed clinical analysis finds that up to 93% of chiropractic billing errors trace directly to incomplete medical necessity documentation. These are not random mistakes — they are structural gaps that repeat claim after claim.
Documentation is the shield. When the documentation holds, claims hold. When it does not, the exposure is not one denied claim — it is a pattern that compounds across every similar encounter in the records.
The 2026 regulatory environment adds pressure on two fronts simultaneously. CMS Medicare conversion factor reductions are compressing reimbursement baselines across all standard spinal manipulation codes, meaning practices collect less per correctly billed claim. At the same time, updated ICD-10 code sets require operational adjustments to avoid diagnostic code denials on claims that would otherwise qualify for payment.
A practice with documentation gaps heading into this environment faces both reduced reimbursement rates and elevated denial risk at the same time.
An internal audit addresses this before it becomes a cash flow problem. The process moves through four sequential phases: Documentation Integrity Review, Modifier and Code Accuracy Sweep, Payer-Specific Denial Pattern Analysis, and Corrective Action and Forward Compliance Plan. The goal is not to pass an audit. It is to make the audit a non-event — because the documentation is already correct.
Last Updated: June 22, 2026
- • Why 2026 Is a Different Kind of Regulatory Pressure for Chiropractic Practices
- • What Automated EHR Scrubbing Misses — and Why It Matters in 2026
- • Why Volume-First Billing Leaves Your Highest-Value Claims Undefended
- • The Four-Phase Internal Audit Process
- • Audit Readiness Checklist: What Your Records Must Show Before 2026
-
• Frequently Asked Questions About Internal Coding Audits Before 2026
- • What is the primary focus of an internal chiropractic coding audit?
- • How often should a chiropractic clinic perform a coding and documentation review?
- • Which Medicare modifiers are most targeted during 2026 audit preparation?
- • Can we rely on our EHR software to catch compliance errors automatically?
- • How does a performance-based billing partner assist with proactive audits?
- • What happens if our practice is audited before we complete an internal review?
- • Your Documentation Is Either a Shield or a Liability — Choose Now
Why 2026 Is a Different Kind of Regulatory Pressure for Chiropractic Practices
Most regulatory years ask for a tweak. A code update. A fee schedule adjustment. You handle it in a staff meeting and move on.
2026 is not that. And the difference isn't volume — it's timing.
CMS Medicare conversion factor cuts are compressing reimbursement baselines across every standard spinal manipulation code. That means less revenue per claim — even when the claim is clean, coded accurately, and fully documented. The floor is dropping regardless of what your practice does right.
And ICD-10 coding updates don't ask for permission. They take effect every October 1 — mandatory diagnostic adjustments that require operational readiness before a single claim hits the payer. Miss the update window and correctly treated patients generate denials on codes that no longer map.
Neither pressure is optional. Both require active preparation before the calendar forces the issue.
The Compounding Risk: When Fee Cuts and Code Changes Hit at the Same Time
Compounding risk doesn't announce itself. It accumulates.
Fee schedule compression makes the math stop working. Code set changes produce denials that look like coder errors — until someone traces them back to a dataset that never got updated. By the time the pattern is visible in the AR, the damage is already done.
A practice earning less per claim while absorbing a spike in diagnostic denials isn't facing two separate problems.
It's facing one accelerating cash flow crisis. And documentation is your shield — the only structural defense standing between those two forces and the practice's bottom line.
Medicare's chiropractic coverage is already a narrow lane. Manual spinal manipulation to correct subluxation — CPT codes 98940, 98941, and 98942 — that's it. Nothing else qualifies.
That narrow window leaves zero margin. Every gap in medical necessity records, every modifier inconsistency, every outdated diagnostic code is a denial you could have prevented. The documentation has to be structurally sound before regulators arrive — not corrected in response to them. That's what it means to defend your practice against audits.
What Practices That Wait Until January Will Face
Practices that wait until January aren't catching up on paperwork. They're attempting to reverse-engineer compliant documentation under active payer scrutiny.
The reimbursement rates are already compressed. The claim backlog is already built on the old code set. Denials are already in motion. At that point, you're not preparing for 2026 — you're responding to it. That's not a tight timeline. That's a structural disadvantage.
That's not an audit risk. That's a structural revenue problem.
The practices that get through 2026 cleanly are the ones that treated the pre-regulatory window as a preparation window — not a grace period.
| Regulatory Change | Effective Date | Primary Impact on Chiropractic Billing | Risk If Unprepared |
|---|---|---|---|
| Medicare Conversion Factor Reduction | Effective January 1, 2026 | Reduces reimbursement baseline across all standard spinal manipulation codes — practices collect less per claim even when documentation is fully correct | Revenue compression on every clean claim filed; no documentation fix can recover the per-claim shortfall if the fee schedule baseline is not updated before billing resumes |
| ICD-10 Diagnostic Code Set Update | Effective October 1 annually (next cycle active for 2026 claims) | Requires operational alignment of diagnostic codes before claims are submitted — outdated codes generate denials on otherwise qualifying services | Spike in diagnostic denials across Medicare and commercial payer claims; denials appear as coder errors until traced back to an unupdated code set |
| AT Modifier Documentation Standard | Ongoing enforcement with heightened OIG audit priority heading into 2026 | Requires consistent, visit-level documentation of active treatment status to support modifier use on every covered spinal manipulation claim | Claims billed without defensible modifier documentation are subject to repayment demands and potential exclusion from future Medicare billing |
| Medicare Coverage Scope (CPT 98940–98942) | Established coverage parameters; compliance scrutiny increasing in 2026 audit cycle | Limits covered chiropractic services to manual spinal manipulation to correct subluxation — all other services require separate, correctly documented billing pathways | Claims billed outside the covered scope — or lacking subluxation documentation — are denied as non-covered and flagged for pattern review |
| Compounding Dual-Pressure Environment | Both pressures active simultaneously beginning Q1 2026 | Fee schedule compression and elevated denial risk arrive together — practices absorb lower per-claim revenue while managing a higher volume of documentation-triggered denials | Practices without a completed internal audit face both pressures at once, with no documentation baseline to defend claims or identify which revenue losses are recoverable |
What Automated EHR Scrubbing Misses — and Why It Matters in 2026
Here's the assumption that costs practices the most going into 2026: the EHR is handling billing.
It isn't. It's handling submission. Those are not the same job.
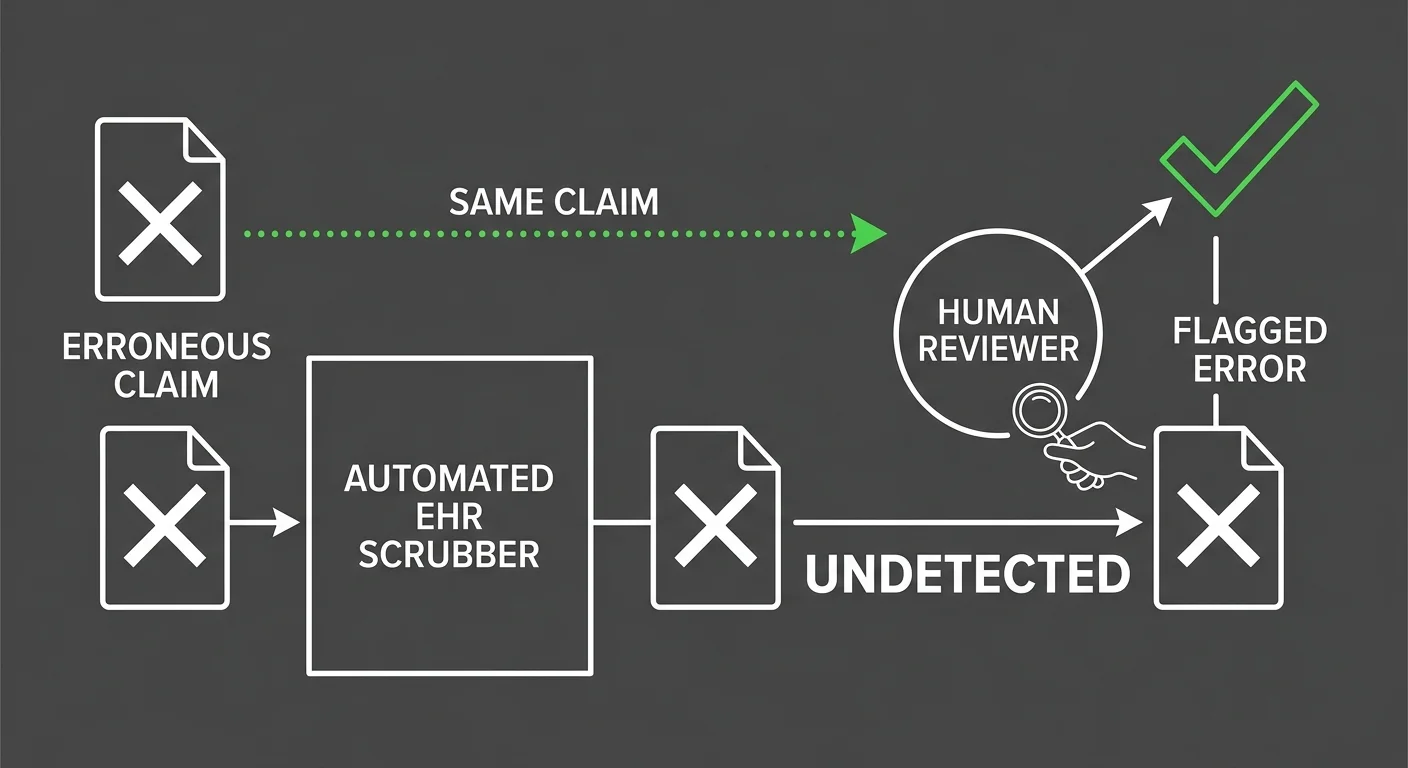
Automated clearinghouse scrubbing catches formatting errors. It flags missing required fields. It confirms a code exists in the system.
But when a claim requires a medical necessity argument — when the documentation has to demonstrate active care, not maintenance, with clinical specificity — the scrubber has no pathway. It passes the claim or drops it. It cannot read the note, evaluate the argument, or identify what's missing before the payer does.
That gap isn't a software limitation a newer platform solves. It's a structural boundary between claim submission and chiropractic billing services that require human clinical judgment.
In 2026, with payer scrutiny elevated across the board, that boundary is exactly where practices lose the most recoverable revenue.
Why the EHR Is a Submission Tool, Not a Billing Solution
The EHR was built to document care and push claims through a clearinghouse. That's the job it was designed for.
But a note that satisfies the clinical record doesn't automatically satisfy the medical necessity standard a payer applies when they're deciding whether to pay or deny. Those are two different bars. The EHR only clears one of them.
So the EHR submits the claim. The payer reviews it. The payer denies it — not because the code was wrong, but because the documented rationale for active treatment didn't hold up.
NIH-analyzed clinical data confirms that up to 93% of chiropractic billing errors trace directly to incomplete medical necessity documentation. The software never flagged it. The note looked complete. The claim was not.
When that denial comes back, the EHR has no recovery pathway.
Someone has to read the note, find the gap, build the appeal, and resubmit with corrected documentation. That's human work. In a volume-first billing setup, it frequently doesn't happen. The claim ages. The revenue is gone.
The Specific Claim Types Your Software Cannot Defend
Automated scrubbing does fine with clean claims — standard codes, straightforward diagnoses, payers with predictable rules. The claims that fail are the ones that require clinical context the scrubber cannot read.
Active treatment modifier documentation. Complex spinal region coding across CPT 98940 through CPT 98942. Personal injury lien billing with multi-payer coordination. These aren't edge cases. For most chiropractic practices, they're the core of the revenue stream — and they're exactly what the scrubber is structurally blind to.
Automated EHR clearinghouse scrubbing misses up to 40% of custom-payer clinical necessity denials. Not the easy claims — the complex ones. The high-value ones. The ones most likely to move the needle on collections.
Those claims pass through the scrubber undetected and land at the payer without the documentation they need. The denial comes back. Nobody works it. It ages.
That pattern shows up in the AR report, in the aging buckets, in the cash flow gap at the end of the month. And when you're already absorbing a compressed reimbursement baseline, managing conversion factor pressure becomes a losing fight if you're also bleeding revenue to unworked denials.
That 40% is not recoverable through better software. It's recoverable through human review — through a Documentation Integrity Review that catches what the scrubber passed, and a Modifier and Code Accuracy Sweep that identifies the pattern before the payer builds a trend file.
The shield doesn't hold because the technology is good. It holds because someone is reading the notes.
| Claim Type | EHR Automated Scrubbing Coverage | Human Review Required | 2026 Audit Exposure Level |
|---|---|---|---|
| Active treatment modifier (AT) documentation | Confirms modifier field is present; cannot evaluate whether clinical notes support active vs. maintenance care distinction | Yes — reviewer must read the note and assess whether documented findings justify active treatment status | High — AT modifier errors are a primary OIG audit target for chiropractic Medicare claims |
| Medical necessity narrative for spinal manipulation | Passes claim if diagnosis code maps to a covered condition; cannot assess whether the clinical rationale is sufficiently documented | Yes — reviewer must verify that objective findings, functional limitations, and treatment goals are explicitly recorded | High — missing or thin medical necessity documentation is the leading driver of chiropractic billing errors in clinical review |
| CPT code selection across 98940–98942 (spinal region count) | Verifies that selected CPT code exists and is on the accepted code list; cannot confirm whether the documented region count matches the billed complexity level | Yes — reviewer must cross-reference the clinical note's documented spinal regions against the submitted CPT code | Moderate to High — miscoded region complexity generates both denials and overpayment recoupment exposure |
| Personal injury lien billing with multi-payer coordination | Can check claim format and required field completion; cannot manage lien priority sequencing, coordination of benefits, or narrative justification across payers | Yes — human coordination required to manage lien documentation, payer sequencing, and case-specific narratives | High — PI lien claims involve non-standard workflows that automated scrubbing is not built to evaluate |
| Updated ICD-10 diagnostic code mapping (2026 code set) | Scrubber validates against its current code library; library must be manually updated after each October 1 release to remain accurate | Yes — reviewer must confirm that the scrubber's active dataset reflects the current code year before claims are submitted | High — claims built on prior-year code sets generate avoidable denials that are invisible until the payer flags them |
| Maintenance care vs. active care documentation distinction | No pathway to evaluate clinical narrative context; passes or drops based on code and modifier field presence alone | Yes — reviewer must assess whether the documented treatment plan and patient response support continued active care billing | High — maintenance care billed as active treatment is a recoupment trigger and a primary compliance exposure point heading into 2026 |
Why Volume-First Billing Leaves Your Highest-Value Claims Undefended
Most billing companies measure success by how many claims go out the door. Not by how much money comes back. Those aren't the same metric. And the gap between them is exactly where chiropractic practices lose the most recoverable revenue.
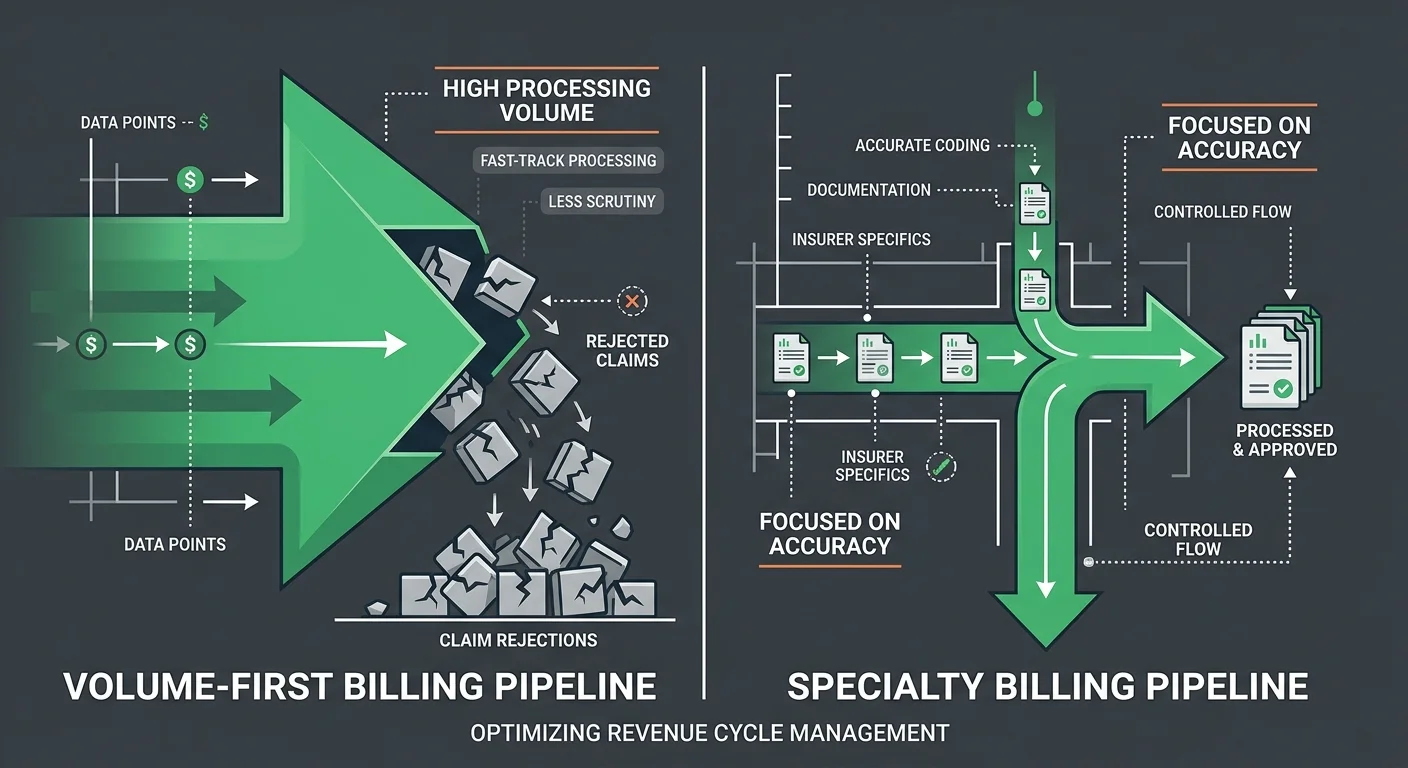
Volume-first billing is built for throughput. Clean claims, fast submission, low cost per transaction. That model works fine when every encounter is textbook-simple.
But the moment a claim requires clinical context — an active treatment modifier argument, a complex spinal region coding decision, a medical necessity rationale that has to hold up under payer review — the volume model has no pathway. It wasn't designed to work those claims. It was designed to move past them.
So the claim goes out incomplete. The payer denies it. And in a high-throughput operation, nobody builds the appeal, corrects the documentation, or resubmits.
Published audit data shows documentation error rates exceeding 80% in targeted AT modifier reviews. Those aren't random failures. They're the predictable output of a billing model that was never designed to work those claims in the first place.
The Volume Model's Structural Blind Spot
Here's why it persists: volume models survive on margin. High claim count, low cost per claim, predictable throughput. Complex claims cost more time to work than the model budgets for. So abandonment isn't a failure of effort — it's the rational economic move.
And the claims that get deprioritized aren't obscure edge cases. They're the highest-value claims in a chiropractic revenue stream — active treatment modifier documentation, CPT 98940, 98941, and 98942 coded with clinical specificity, personal injury lien billing with multi-payer coordination.
Peer-reviewed clinical analysis confirms that up to 93% of chiropractic billing errors trace directly to incomplete medical necessity documentation. That's the precise gap a volume-first model is structurally unable to close — because closing it costs time the model never budgeted.
But the blind spot runs deeper than abandoned appeals. When complex claims fail repeatedly — same modifier, same documentation gap, same payer — the volume model doesn't surface the pattern.
There's no one reading the denial trend file. No one connecting claim type to failure rate. The weekly communication framework that would catch these patterns and route them to intervention simply doesn't exist in a throughput-first operation.
The shield has gaps. And no one is tracking where they are.
This Isn't for Every Practice — Know Where You Stand
This isn't a message for every practice. If your billing is clean, your denial rate is low, and your AR is current — this isn't your problem right now. That's a strong position. The internal audit process described here is about protecting it going into 2026, not recovering from a wreck.
But if rate is your primary decision criterion — if the first question is what's the fee and the process conversation never really happens — the volume model is probably where you'll land.
Bushido Billing isn't the right fit for that conversation. The work here is built around revenue recovery and clinical documentation integrity. That's a different product than lowest-cost submission. Both exist. They don't serve the same practice.
What volume-first billing can't provide is the human judgment that makes high-complexity claims defensible. Practices that need a billing partner to stay invisible — no documentation cooperation, no provider availability for appeals, zero engagement — will get exactly what that model produces.
What they won't get is a functional shield between their highest-value claims and the 2026 regulatory environment. That shield requires someone who reads the notes.
| Billing Approach | Claim Prioritization Logic | AT Modifier Handling | PI Lien Handling | Revenue Recovery on Complex Claims |
|---|---|---|---|---|
| Volume-First / Automation-Forward | Clean claims first — high-throughput, low cost per transaction; complex claims deprioritized when they require more time than the model budgets | Passed or dropped by clearinghouse scrubber with no human review of the underlying clinical argument; modifier errors reach the payer undetected | Structurally underserved — multi-payer coordination and lien documentation require case-level human judgment the volume model does not provide | Low — complex claims that require appeal, documentation correction, or medical necessity arguments are frequently abandoned rather than worked |
| Generalist Billing (Multi-Specialty) | All specialties treated equally — chiropractic-specific rules applied inconsistently because the billing team lacks vertical depth across AT modifier and maintenance vs. active care standards | Applied generically without specialty-level knowledge of Medicare active-care documentation requirements; miscoding of spinal regions across CPT 98940–98942 goes unreviewed | Inconsistent — personal injury lien workflows fall outside standard generalist training; coordination errors compound across payer parties | Unpredictable — revenue recovery depends on whether a given claim fits a template the generalist team already knows, not on clinical specificity |
| EHR-Native Submission (No Dedicated Billing Partner) | Submission-only model — the EHR moves claims through a clearinghouse but has no mechanism to review, appeal, or correct what the payer returns | No active oversight — the modifier is applied at the point of documentation entry; if the clinical note does not satisfy active-care standards, the error travels through submission to denial without interception | Not supported — PI lien billing requires coordination logic and timeline management that EHR platforms do not provide | Minimal — denial management and AR recovery require human follow-up that the EHR cannot perform; revenue loss compounds as denials age |
| Performance-Based Embedded Billing Partner (Chiropractic Specialty) | Revenue recovery drives prioritization — complex, high-value claims receive the same attention as clean claims because the model's economics depend on what actually gets paid, not what gets submitted | Human-reviewed at the documentation level before submission; active-care vs. maintenance distinction evaluated against clinical notes, not just code fields | Supported through dedicated case management — multi-payer coordination, lien timelines, and documentation requirements tracked as a structural workflow, not an exception | High — appeals are built, documentation gaps are corrected, and denial patterns are tracked and reported so the same failure does not repeat across the claim set |
The Four-Phase Internal Audit Process
So what does the actual work look like?
Four sequential phases. Each one closes a specific gap that automated scrubbing can't close — and that payer scrutiny will absolutely find.
These phases aren't a checklist you run once and file away. They're a systematic sweep — documentation integrity, modifier accuracy, denial patterns, forward compliance posture.
Skip any one of them and the shield has a gap. Payer scrutiny in 2026 is specifically designed to find those gaps.
Here's how each phase works.
Phase 1: Documentation Integrity Review
The Documentation Integrity Review starts at the note level. Not the claim level.
Most practices find documentation problems after a denial lands. This phase finds them before the claim ever leaves the practice.
Each note gets evaluated against one question: does it substantiate active care with the specificity a payer demands during medical necessity review? That means documented functional limitations, measurable treatment goals, and a clear clinical rationale for why ongoing manipulation is actively therapeutic.
Not maintenance. The active versus maintenance care distinction is where the most recoverable dollars quietly disappear — and where Phase 1 starts pulling them back.
Medicare coverage is narrower than most practices assume. It applies specifically to manual spinal manipulation to correct subluxation under CPT codes 98940, 98941, and 98942. That's the window. It doesn't flex.
Every note in this phase gets measured against that standard — not in general terms, but in the specific clinical language a payer reviewer evaluates line by line.
Phase 2: Modifier and Code Accuracy Sweep
The Modifier and Code Accuracy Sweep is where documentation integrity meets billing execution. A note can be clinically complete and still produce a denial if the modifier selection doesn't match what the note actually says.
This phase cross-references every active therapeutic modifier against the supporting documentation. Claim by claim. Not a batch sample.
AT modifier accuracy is the highest-risk variable heading into 2026. OIG audit data shows documentation error rates exceeding 80% in targeted AT modifier reviews.
Those aren't random failures scattered across claim types. They concentrate in complex spinal region coding decisions — the active versus maintenance distinction, the appropriate region count across CPT 98940–98942, the modifier logic that has to hold up under a payer's retrospective review.
So this phase isn't looking for typos. It's looking for structural mismatches.
Where the clinical note supports one level of care and the modifier reflects another. Where the spinal region count doesn't align with the documented treatment area. Where the code is technically valid but clinically unsupported.
Those mismatches are what regulators are trained to find. The sweep finds them first.
Phase 3: Payer-Specific Denial Pattern Analysis
The Payer-Specific Denial Pattern Analysis is the phase most internal audits skip.
Reading denial data as a pattern — not as a queue of individual problems — takes more than a clearinghouse report. But patterns are exactly what 2026 payer scrutiny is built to surface.
This phase pulls denial data by payer, by code, and by denial reason — then reads across that data for what's recurring.
A single denial on a complex spinal coding decision is a claim problem. Ten denials on the same code type from the same payer, all citing the same documentation deficiency, is a trend file that payer is already building.
Recognizing that distinction before the payer acts on it is the difference between a correctable pattern and an audit trigger.
The analysis also catches payer-specific rule variations that generic billing workflows miss entirely. What one payer accepts as sufficient medical necessity documentation, another rejects as incomplete. Those differences don't show up in clearinghouse scrubbing. They show up in denial patterns.
And with CMS conversion factor pressure already compressing fee schedule baselines across all spinal manipulation codes, a denial pattern that was manageable at full reimbursement becomes a structural revenue problem when rates drop.
Phase 4: Corrective Action and Forward Compliance Plan
The Corrective Action and Forward Compliance Plan is where the audit stops being a snapshot and starts being a shield.
The first three phases identify what's broken. This phase determines how to close those gaps before 2026 makes closing them more expensive.
Corrective action means two things at once. Fixing the existing documentation deficiencies across claims that are still workable. And changing the upstream processes that produced those deficiencies in the first place.
One without the other just clears the backlog and rebuilds it.
That's what the forward compliance plan locks in — operational changes to documentation workflows, modifier review checkpoints, and denial escalation paths that make the next internal audit shorter and the next regulatory review less consequential.
The goal of Phase 4 isn't to declare the practice compliant. It's to build the internal discipline that keeps update chiropractic fee schedules current, documentation tight, and the shield in place without waiting for a crisis to trigger it.
| Audit Phase | What You Review | Common Failure Found | Corrective Output |
|---|---|---|---|
| Documentation Integrity Review | Individual clinical notes against active care standards — functional limitations, measurable treatment goals, and documented rationale for ongoing manipulation | Notes that describe care in general terms without substantiating medical necessity — present at the visit level but absent at the clinical detail level payers evaluate | Revised note templates and documentation checkpoints that force specificity before claims are submitted, not after they are denied |
| Modifier and Code Accuracy Sweep | Every active therapeutic modifier against its supporting clinical note — cross-referenced claim by claim, with spinal region counts checked against documented treatment areas | Structural mismatches where the note supports one level of care and the modifier reflects another — or where CPT code selection doesn't align with the documented clinical picture | A modifier review protocol that catches active-versus-maintenance discrepancies before submission and flags spinal region coding decisions for human review |
| Payer-Specific Denial Pattern Analysis | Denial data organized by payer, by code, and by stated denial reason — read across the dataset to identify recurring patterns rather than isolated claim failures | Recurring denials on the same code type from the same payer citing the same documentation deficiency — a trend file the payer is already building while the practice resolves claims individually | A payer-specific rule map that surfaces documentation thresholds by carrier and reroutes complex claims to the appropriate review pathway before submission |
| Corrective Action and Forward Compliance Plan | Both the existing documentation deficiencies across still-workable claims and the upstream processes that produced those deficiencies in the first place | Practices that clean the backlog without changing the workflow — resolving current exposure while rebuilding the same gap in the next billing cycle | Operational changes to documentation workflows, modifier review checkpoints, and denial escalation paths that hold the shield in place without requiring a future crisis to trigger corrective action |
Audit Readiness Checklist: What Your Records Must Show Before 2026
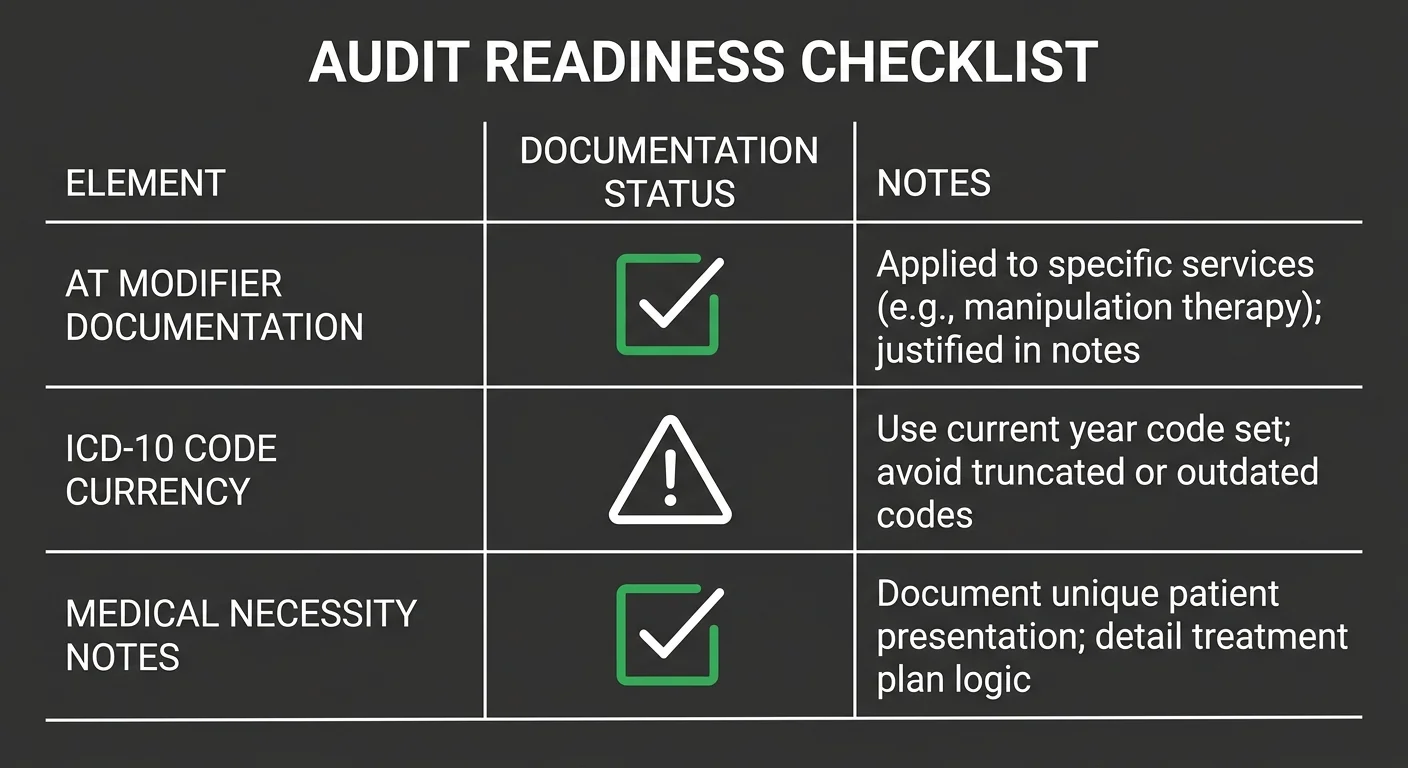
The four phases show you where the gaps are. This section shows you what payer reviewers will actually be looking for when they open your records.
This is the floor. Not a best-practice aspiration — the minimum standard payer reviewers apply when they evaluate your records.
Peer-reviewed clinical analysis confirms that up to 93% of chiropractic billing errors trace directly to incomplete medical necessity documentation. That number doesn't describe a fringe problem. It defines exactly what this checklist is built to close.
Two categories carry the most regulatory risk heading into 2026: AT modifier and medical necessity documentation, and ICD-10 code currency.
Both have clear, auditable benchmarks. Both are exactly where automated scrubbing consistently falls short. And both are where documentation is your shield — or it isn't.
AT Modifier and Medical Necessity Documentation Standards
Here's the standard: every note attached to a Medicare spinal manipulation claim must justify active therapeutic care on its own. Not across a treatment episode. Per visit.
The note must document measurable functional limitations, a time-bound treatment goal, and a clinical rationale that distinguishes this visit from maintenance care. That distinction is exactly what the AT modifier is certifying.
Medicare coverage applies specifically to manual spinal manipulation to correct subluxation, billed under CPT codes 98940, 98941, and 98942. That's the coverage window — it doesn't flex.
The documented spinal regions must align with the CPT code selected. That alignment has to hold under a retrospective review where a payer examines the note, the code, and the modifier at the same time. A note that's clinically complete but coded at the wrong region count fails that review. So does a modifier certifying active care when the note describes a maintenance plateau.
So the readiness standard here is specific: every active claim must have a note that stands alone. No cross-referencing prior visits to establish necessity. No generic functional status language a reviewer can't independently evaluate.
The note is the claim. If the note doesn't hold, the claim doesn't hold.
ICD-10 Code Currency and SDOH Requirement Preparedness
CMS updates ICD-10 diagnostic datasets annually on October 1. That's not a soft deadline — it's the date after which claims billed with retired or superseded diagnostic codes become denial candidates.
Practices that skip an active code currency review before that date are carrying exposure they won't discover until a denial pattern is already established in the payer's system. By then, the damage compounds quietly.
The 2026 ICD-10 cycle introduces expanded social determinants of health coding requirements that intersect directly with chiropractic documentation. These aren't optional additions.
Some Medicare Advantage and commercial plans are already embedding SDOH codes into medical necessity criteria. A practice that hasn't mapped its current diagnostic coding workflow against the updated October 1 requirements isn't running on this year's standards. It's running on last year's shield.
The readiness standard here is currency, not completeness. The question isn't whether your practice uses ICD-10 codes — it's whether those codes reflect the active 2026 dataset and whether the documentation behind each code is specific enough to satisfy updated payer criteria.
Generalist billing workflows don't track payer-specific ICD-10 enforcement shifts. Specialty-level oversight does. That's the difference between a code that clears scrubbing and a code that survives a retrospective review.
| Documentation Element | 2026 Standard Required | Common Gap Found in Audits | Corrective Action |
|---|---|---|---|
| Per-Visit Medical Necessity Statement | Each note independently justifies active therapeutic care — measurable functional limitations, time-bound treatment goal, and clinical rationale distinguishing the visit from maintenance | Generic functional status language carried forward from prior visits; no independent justification per encounter | Rewrite note templates to require visit-specific functional findings and explicit active care rationale before the claim is submitted |
| AT Modifier Documentation Alignment | The modifier selection reflects the exact level of active versus maintenance care documented in the clinical note — no mismatches between what the note says and what the modifier certifies | Modifier applied routinely without confirming the note supports active care; spinal region count in the note does not match the CPT code selected | Cross-reference every modifier against the supporting note during the Modifier and Code Accuracy Sweep before finalizing claims |
| CPT Code and Spinal Region Alignment | The billed CPT code (98940, 98941, or 98942) matches the number of spinal regions documented as treated in the clinical note | Region count in the note is vague or defaulted to a standard template; CPT code selected does not reflect what was clinically documented | Establish a documentation checkpoint requiring region-specific treatment notation before code selection is finalized |
| ICD-10 Code Currency | All diagnostic codes reflect the active CMS dataset in force as of October 1 of the current plan year — no retired or superseded codes on active claims | Diagnostic codes carried forward from prior plan years without review; codes flagged by payers as retired still appearing on current claims | Run a full ICD-10 currency sweep against the updated October 1 dataset before the new plan year opens; flag and replace any retired codes in active templates |
| Social Determinants of Health (SDOH) Coding Readiness | Documentation workflow maps current patient intake data against 2026 SDOH coding requirements for payers enforcing expanded medical necessity criteria | SDOH coding treated as optional; intake documentation does not capture the data elements required by updated Medicare Advantage and commercial payer criteria | Audit intake forms and note templates against the 2026 SDOH requirements during the Documentation Integrity Review and update before the October 1 effective date |
| Payer-Specific Medical Necessity Thresholds | Clinical documentation meets the specific medical necessity language and threshold required by each payer — not a single generic standard applied across all contracts | One universal note template applied to all payers regardless of individual contract requirements; payer-specific documentation criteria not tracked or operationalized | Use denial pattern data from the Payer-Specific Denial Pattern Analysis to map each payer's actual documentation requirements and update templates accordingly |
| Retrospective Review Survivability | Every note can stand alone under retrospective payer review — no dependency on prior visit records to establish necessity, no cross-referencing required to complete the clinical picture | Notes written as continuation of prior visits; necessity implied by treatment history rather than independently established per encounter | Implement a self-contained note standard as part of the Corrective Action and Forward Compliance Plan — each note complete, independent, and defensible in isolation |
Frequently Asked Questions About Internal Coding Audits Before 2026
The process makes sense on paper. But the questions that actually keep practice owners up at night are different — messier, more specific, more urgent.
Here are the ones that come up most. Straight answers. No hedging.
What is the primary focus of an internal chiropractic coding audit?
Medical necessity documentation. That's where the exposure lives.
Peer-reviewed clinical analysis finds that up to 93% of chiropractic billing errors trace to incomplete necessity documentation. The audit verifies one thing: can every active claim stand on its own note? No borrowed language. No cross-referenced visits.
Modifier accuracy and code currency follow from that foundation. But if the note doesn't hold, nothing else does either.
How often should a chiropractic clinic perform a coding and documentation review?
At minimum, once before every major regulatory cycle. That means right now — before the 2026 ICD-10 and Medicare updates take effect.
But a single annual review isn't a shield. It's a snapshot. Practices with embedded billing partners run rolling denial pattern reviews throughout the year. That cadence catches drift before it becomes a pattern payer reviewers can build a case around.
Which Medicare modifiers are most targeted during 2026 audit preparation?
The AT modifier. It's the primary target — and the highest-risk variable heading into 2026.
OIG audit history shows documentation error rates exceeding 80% in targeted AT modifier reviews. That modifier certifies active therapeutic care on every Medicare spinal manipulation claim billed under CPT codes 98940, 98941, and 98942.
If the note doesn't independently justify active care for that specific visit, the modifier fails. And a failed modifier pattern is exactly what a targeted audit is built to surface.
Can we rely on our EHR software to catch compliance errors automatically?
No.
Automated EHR clearinghouse scrubbing misses up to 40% of custom-payer clinical necessity denials. The system checks code structure — it does not read clinical logic. It won't flag a note that's grammatically complete but medically insufficient. It won't catch an AT modifier attached to documentation that describes a maintenance plateau.
Automation processes what it can process. The claims that require clinical judgment are the ones it passes through. Those are also the ones that come back as denials.
How does a performance-based billing partner assist with proactive audits?
A performance-based billing partner loses money when you lose money. That's not a marketing line — it's the structural reason proactive audit work gets done.
That alignment drives modifier review before claims go out. It drives active denial pattern tracking. It means someone is reading the documentation on the AT modifier decisions, the personal injury lien requirements, and the payer-specific necessity standards that automated scrubbing never touches.
There's a real difference between a billing relationship that submits claims and one that defends them. Most practices don't discover which one they have until after the first denial wave.
What happens if our practice is audited before we complete an internal review?
An incomplete audit is still better than no audit. That's not a consolation — it's how audits and enforcement actually work.
Practices that get reviewed with zero prior internal documentation have no record of their own compliance posture. Everything is exposure. But what you've already reviewed and corrected is defensible. Document exactly where your internal review stands at the time of any audit — what was covered, what was corrected, what's still in progress.
Payer reviewers and federal auditors respond to demonstrated good faith. A documented, in-progress review is evidence of exactly that. Partial corrective action on record is not the same as none at all — and the difference between those two positions is not small.
Your Documentation Is Either a Shield or a Liability — Choose Now
Here's what 2026 is actually deciding: documentation is your shield, or it's a liability you haven't priced yet.
There is no middle position.
A practice that ran the full audit — Documentation Integrity Review, Modifier and Code Accuracy Sweep, Payer-Specific Denial Pattern Analysis, Corrective Action and Forward Compliance Plan — holds a shield tested against the exact standards payer reviewers will apply. A practice that skipped it holds an assumption.
But the sharper line isn't between practices that audited and practices that didn't. It's between practices that treated the audit as a drill and practices that treated it as a structural financial defense.
A drill produces a report. A structural defense produces changed documentation workflows, corrected modifier checkpoints, and denial escalation paths that hold without a crisis to trigger them.
That operational discipline is what the shield actually is. Not a one-time review. A practice that produces defensible documentation as a matter of course — because the process demands it, not because an auditor showed up.
The 2026 regulatory changes don't create new vulnerabilities. They expose the ones that have always been there.
Incomplete medical necessity documentation. AT modifier mismatches. Outdated diagnostic codes. These aren't 2026 problems — they're existing gaps that an updated enforcement environment will make significantly more expensive to ignore.
Practices that have done this work are ready. Bushido Billing exists for the practices that recognize what this moment requires — specialty-level oversight that volume-first, automation-forward workflows structurally cannot provide, and a performance-based model that aligns every incentive around revenue recovery.
The shield gets built through human review, clinical specificity, and a billing partner who actually reads the notes. The question isn't whether you need it going into 2026. The question is whether you're building it now — or waiting until the first denial wave shows you exactly where your documentation failed.
You've read this far because the 2026 deadline is real and you know your documentation isn't where it needs to be. That gap doesn't close on its own. It compounds. If you want to see exactly where your practice stands before the first denial wave hits, Book a Call with Bushido Billing. One conversation tells you what's defensible — and what isn't.

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet