

What Are the New ICD-10 Social Determinants of Health (SDOH) Codes for Chiropractors in 2026?
The 2026 ICD-10 Social Determinants of Health (SDOH) codes for chiropractors are non-payable diagnosis codes drawn from the Z55–Z65 code blocks, maintained by the CDC's National Center for Health Statistics. They document the socioeconomic and environmental factors — housing instability, food insecurity, transportation barriers, financial strain, and social isolation — that directly shape a patient's clinical presentation and recovery.
They do not generate a reimbursement line. That is the fact most practices get wrong.
SDOH codes are documentation tools, not billing tools. That distinction changes everything about how to use them. When a patient cannot reliably access home-based care alternatives because of a documented transportation barrier, the Z-code turns that context into a codified, auditable fact in the medical record. A Z-code is not a revenue line — it is a structural argument for medical necessity.
CMS is actively tracking Z-code utilization patterns at the regional level to assess both health equity initiatives and clinic-level audit risk. Practices that have consistently skipped SDOH documentation are now visible in that data — not because they did anything wrong, but because the absence of documentation is itself a signal.
Historically, fewer than 2% of chiropractic encounters included SDOH codes. That gap is now a liability.
Under CMS finalized guidelines, any member of the healthcare team — including front-desk and support staff — can collect SDOH data, as long as the clinician verifies it and it is entered in the patient's medical record. Implementation does not require a complete workflow overhaul. It requires a deliberate process.
For chiropractic practices navigating 2026 Medicare requirements, SDOH codes are not optional overhead. They are the structural layer that makes a billing file defensible under audit.
Last Updated: June 22, 2026
- • What Are ICD-10 SDOH Codes — and Why Chiropractors Are Finally Being Watched
- • Why Volume-First Billers Ignore Z-Codes (And What That Costs You)
- • The 2026 ICD-10 SDOH Code Set Chiropractors Need to Know
- • How to Document SDOH Codes Without Slowing Down Your Front Desk
-
• Frequently Asked Questions
- • What are the new 2026 ICD-10 SDOH codes for chiropractors?
- • Why is Medicare auditing chiropractic SDOH code documentation?
- • Does a chiropractor need a formal diagnosis to bill a Z-code?
- • How do SDOH Z-codes affect clinical reimbursement rates?
- • Can chiropractic office staff document social determinants of health?
- • Z-Codes Are Load-Bearing Walls — Build Them Into Your Billing Now
What Are ICD-10 SDOH Codes — and Why Chiropractors Are Finally Being Watched
Most chiropractors have heard of Z-codes. Very few have been told what CMS is now doing with them in 2026.
ICD-10 Social Determinants of Health codes live inside the Z55–Z65 code blocks. They're non-payable — meaning no revenue line attaches directly to them. What they do is document the socioeconomic and environmental conditions shaping how a patient heals. Or fails to.
Housing instability. Food insecurity. Transportation barriers. Financial hardship. Social isolation.
These aren't soft observations. They're clinically codified facts that explain why a patient's recovery looks the way it does. And they're exactly what an auditor looks for when active care needs justification.
A Z-code is not a revenue line — it is a structural argument. Think of it as the load-bearing wall inside a billing file. Invisible from the outside. But the reason the whole structure holds when audit pressure arrives.
Practices that skip SDOH documentation are not just missing codes. They are pulling out the structural supports from their own files.
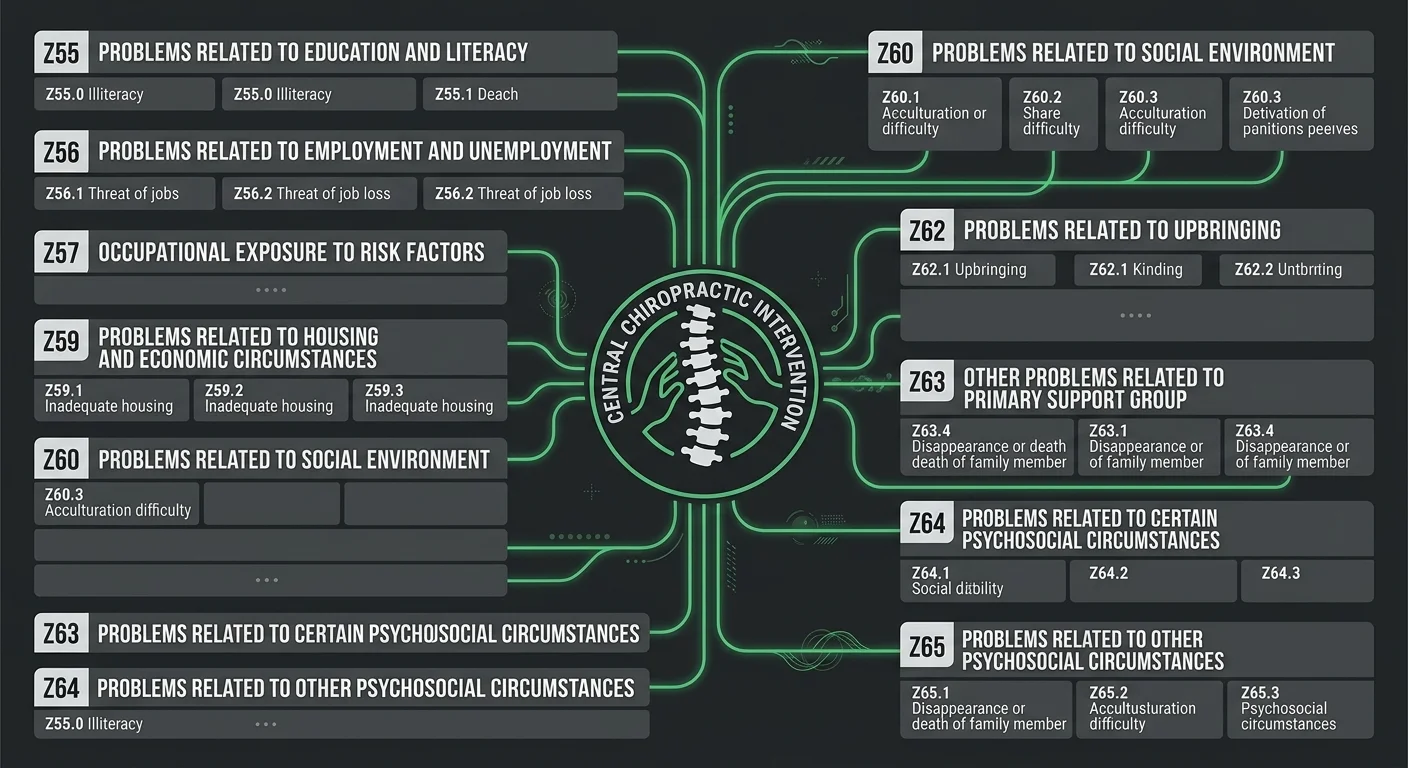
The Z55–Z65 Code Block Explained
The CDC maintains the Z55–Z65 code blocks as the official ICD-10-CM classification system for socioeconomic factors that influence clinical outcomes. Ten code blocks. Each one targeting a distinct layer of the patient's non-medical reality.
Z55 opens with problems related to education and literacy. The blocks move through social environment, housing, economic circumstances, and employment. Z65 closes with psychosocial circumstances affecting overall health status.
That's the full architecture. And most chiropractic practices have documented almost none of it.
For chiropractic, the codes that matter most are the ones that document access and compliance barriers. Z59 covers housing and economic problems. Z60 addresses social environment factors. Z63 and Z65 capture the household and psychosocial stressors that show up repeatedly in chronic musculoskeletal presentations.
These are the codes that answer the auditor's real question: why did this patient need active, in-office care instead of a home-based alternative?
If your file can't answer that question, your claim can't survive scrutiny.
Here's what most practices get wrong: SDOH codes don't require a formal medical diagnosis. They require documented observation — an identified barrier, verified by the clinician, entered into the record.
Published analysis confirms that any member of the healthcare team can collect this data, including front-desk and support staff, as long as the clinician signs off and it's entered in the medical record.
The process doesn't need to be clinical. It needs to be consistent.
Why CMS Tied SDOH Reporting to Medicare Quality Metrics in 2026
CMS is now tracking Z-code utilization patterns at the regional level — using them to evaluate both health equity initiatives and clinic-level audit risk. This isn't a proposed rule or a future policy. It's a live data signal running right now.
Practices that have consistently left Z-codes blank are already visible in that data.
The absence of SDOH documentation isn't neutral. It's a pattern. And when CMS quality metrics flag Z-code gaps as risk vectors, practices that never used these codes aren't flying under the radar.
The gap itself is the signal.
Don't wait until that signal becomes the subject of Medicare compliance review to find out what's missing from your files.
Practices that invest in full-service insurance billing understand that SDOH coding isn't overhead to absorb. It's a documentation layer that anchors the entire revenue protection strategy.
Bushido Billing builds this layer in from the start. Not as an add-on. As a structural feature of how claims get built.
The practices that master SDOH coding now are building audit-proof files. Everyone else is still treating Z-codes as optional checkboxes — and they'll find out what that costs when audit season arrives.
| SDOH Category | ICD-10 Z-Code Range | What It Documents | Relevance to Chiropractic |
|---|---|---|---|
| Housing and Economic Problems | Z59 | Documents housing instability, inadequate housing, lack of adequate food, extreme poverty, and low income — factors that limit a patient's ability to follow through on home-care recommendations | Supports medical necessity for in-office adjustments when a patient cannot reliably self-manage or access home-based alternatives due to documented economic constraints |
| Social Environment Factors | Z60 | Documents social isolation, problems related to living alone, acculturation difficulty, and exclusion or rejection — conditions that affect recovery motivation and care compliance | Explains reduced treatment adherence and provides clinical context for why active, supervised care produces better outcomes than home exercise programs alone |
| Education and Literacy | Z55 | Documents problems with literacy, schooling, and education level — barriers that affect a patient's ability to understand and execute a home care protocol | Validates the need for hands-on clinical instruction and in-office supervision rather than written or self-directed rehabilitation plans |
| Employment and Occupational Circumstances | Z56–Z57 | Documents unemployment, job loss, exposure to occupational risk factors, and physically demanding work conditions contributing to musculoskeletal stress | Establishes the external physical stressors driving the clinical presentation — strengthening the medical necessity argument for ongoing chiropractic care |
| Family and Psychosocial Circumstances | Z63 and Z65 | Documents family relationship problems, household stressors, and other psychosocial circumstances — including exposure to disaster, civil conflict, and problems related to legal circumstances | Captures the chronic psychosocial load that slows musculoskeletal recovery and explains why a patient's case history extends beyond a straightforward mechanical injury |
| Transportation and Access Barriers | Z59.8 (within Z59 block) | Documents barriers to accessing healthcare, including lack of transportation and geographic or logistical obstacles to consistent care attendance | Directly reinforces why in-office chiropractic care is the most clinically appropriate option — and defends visit frequency against payer challenges on maintenance vs. active care grounds |
Why Volume-First Billers Ignore Z-Codes (And What That Costs You)

Most billing operations skip Z-codes entirely. Not by accident. By design.
Volume-first billers measure performance by claims out the door. Speed is the metric. Documentation depth isn't. Non-payable codes slow the queue, so they get dropped. It's a rational decision inside a broken model.
NIH peer-reviewed analysis puts a number on that pattern: historically, fewer than 2% of chiropractic encounters used SDOH codes. That's not a minor gap. That's a documentation deficit large enough to register in CMS quality metrics — and CMS is actively using Z-code utilization patterns to assess clinic-level audit risk. The gap isn't invisible. It's the signal.
The Volume Model's Fatal Flaw: Non-Payable Doesn't Mean Worthless
Here's the core misunderstanding: non-payable does not mean worthless. A Z-code doesn't generate a reimbursement line. But it builds the structural argument that justifies every reimbursement line in the file.
Volume models deprioritize anything that doesn't produce an immediate billing result. That logic works on clean, straightforward claims. It falls apart the moment a payer questions medical necessity.
Without SDOH documentation, a chiropractic billing file can't answer the auditor's real question: why did this patient need frequent, in-office active care instead of a home-based alternative? The claim submits. The file looks thin. When an auditor asks why this patient needed twelve visits instead of three, there's no codified answer in the record.
That's where practices relying on generalist billing start losing revenue. Not at submission. At the audit triggers for unspecified diagnosis codes stage — when the file is expected to make sense on its own and can't. CMS isn't counting claim volume. It's evaluating whether the documentation holds. And with 2026 audit pressure intensifying, Z-codes are no longer optional context. They're part of the required answer.
Who This Approach Isn't Built For
This approach isn't built for practices that want billing running quietly in the background with zero provider involvement. That model produces exactly the documentation gaps that 2026 audit pressure is designed to surface. Minimal engagement means a thin file. A thin file means exposure.
And if the first question in a billing conversation is about rate — not process, not communication, not specialty knowledge — SDOH coding will never enter the workflow. It takes deliberate implementation, clinician sign-off, and a billing partner who treats non-payable codes as revenue protection tools. Not overhead to skip.
Bushido Billing is built for practices that know the difference between a billing company that submits claims and an embedded billing partner that builds defensible files. If you need volume and speed, this isn't the right fit. If you need documentation that holds under the regulatory scrutiny 2026 is bringing, that's a conversation worth having.
| Billing Model | Z-Code Treatment | Audit Exposure | Revenue Impact |
|---|---|---|---|
| Volume-first generalist biller | Dropped from workflow — non-payable codes slow claim queue throughput | High — documentation gaps are visible in CMS quality metrics tracking; absence of Z-codes is itself a risk signal | Claims submit but fail under medical necessity scrutiny; revenue lost at audit stage, not submission |
| EHR platform (self-managed) | Ignored — EHR software processes payable codes; non-payable Z-codes require human judgment to select and document correctly | High — no structural argument built into the file; payer questions on visit frequency go unanswered in the record | Clean claims paid; complex claims denied when documentation cannot justify active care over lower-intensity alternatives |
| Generalist biller with chiropractic clients | Inconsistent — Z-codes applied only when recognized, not as a systematic documentation layer | Moderate to high — uneven coding patterns create irregular audit footprints that attract scrutiny | Partial revenue protection; practices exposed on exactly the high-value, high-complexity claims that require the strongest files |
| Embedded billing partner — chiropractic specialist | Integrated — SDOH codes are built into the documentation workflow as a standard layer, not an optional add-on | Low — Z-code presence creates a structural argument for medical necessity that survives audit review | Revenue protected at the file level; documentation supports every reimbursement line, including high-frequency active care plans |
The 2026 ICD-10 SDOH Code Set Chiropractors Need to Know
The Z55–Z65 code blocks are the ICD-10-CM classification system for socioeconomic factors that directly shape clinical outcomes. Ten distinct blocks. Each one targeting a different layer of the patient's non-medical reality — education, housing, employment, economic hardship, psychosocial stress.
For chiropractic practices, these aren't abstract categories. They describe the exact circumstances showing up in active care caseloads every week.
Knowing the code set exists is not enough. Knowing which codes apply to chiropractic workflows — and why — is what turns SDOH documentation into a billing defense strategy.
The full Z55–Z65 spectrum maintained by the CDC spans ten distinct blocks. Not all of them are equally relevant to chiropractic. But for practices building defensible active care records, a focused subset carries the most weight.
The new ICD-10 SDOH codes for chiropractors that matter most in 2026 billing defense cluster around housing stability, transportation access, economic hardship, social support deficits, and occupational barriers. These are precisely the factors that explain why a patient's musculoskeletal recovery timeline looks the way it does — and why the care plan is what it is.
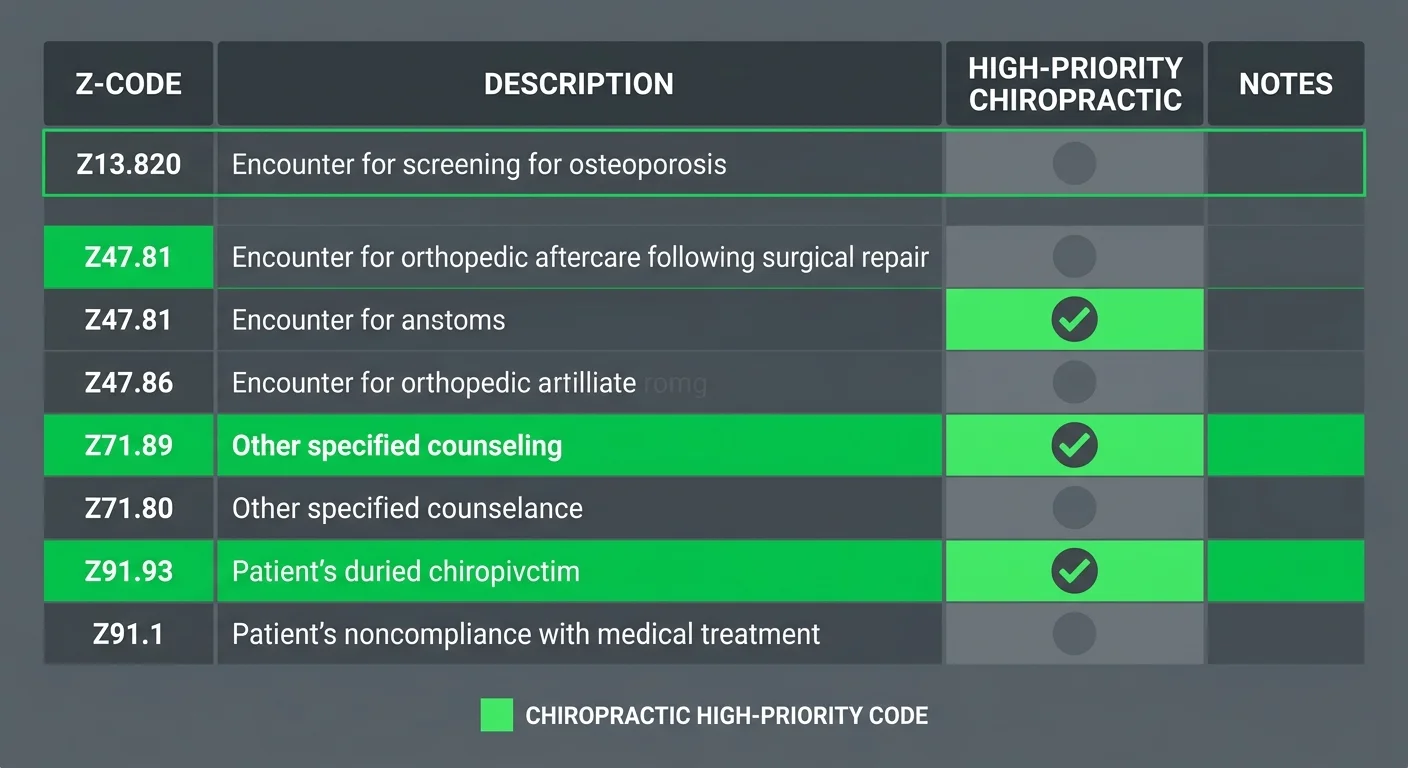
High-Priority Z-Codes for Chiropractic Active Care Documentation
Z59 covers housing instability and economic problems — directly relevant when a patient's living environment is contributing to a physical condition or preventing consistent recovery. Z60 addresses social environment factors, including isolation and adjustment difficulties that affect whether a patient can realistically follow through on treatment.
Z63 captures family and household stressors that surface consistently in chronic musculoskeletal cases. Z56 documents occupational demands that make home-based alternatives clinically inadequate.
Each code is a specific answer to a specific auditor question. Document it now or explain the gap later.
Transportation barriers sit inside Z59 — and they're one of the most directly applicable codes for chiropractic active care justification.
When a patient lacks reliable transportation, frequent in-office adjustments aren't a billing preference. They're the clinically supported decision. Documenting that barrier transforms an abstract care frequency choice into a codified necessity argument. The record makes the case so you don't have to make it later under pressure, in a payer audit, against a reviewer who's looking for any reason to reduce the claim.
None of these codes require a formal medical diagnosis. They require documented observation — a barrier identified, verified by the clinician, entered in the record.
That's it. The threshold is achievable. What breaks it is inconsistency, not complexity.
How SDOH Codes Strengthen Medical Necessity Arguments
Here's what most billing operations miss: SDOH codes don't add revenue to a claim. They protect the revenue already in it.
When environmental variables go undocumented, the billing file has no structural explanation for why a patient's recovery required the level of care it did. The claim submits. The file can't defend itself. Those are two very different things.
Non-payable does not mean worthless. A Z-code is the load-bearing wall of a medical necessity argument. It is the codified reason why twelve visits was the right clinical decision instead of three.
When a payer or auditor questions care frequency, the practice that documented transportation barriers, housing instability, or economic hardship has an answer built into the record. The practice that skipped those codes does not.
That gap is exactly what surfaces in a billing audit. Thin documentation is the trigger — not the diagnosis itself.
Documented barriers validate why active, in-office care with frequent adjustments is clinically necessary over home-based alternatives. The logic holds because the record holds.
When socioeconomic and environmental factors are codified into the file, the care plan isn't an inference. It's a documented argument. One that stands on its own when regulatory scrutiny arrives — and in 2026, it will arrive.
| Z-Code | Description | Documentation Trigger | Medical Necessity Argument Supported |
|---|---|---|---|
| Z55 | Problems related to education and literacy | Patient reports difficulty understanding home exercise instructions or written care plan materials | Justifies increased in-office supervised treatment frequency over self-directed home care alternatives |
| Z56 | Problems related to employment and unemployment | Patient documents physically demanding occupation, irregular hours, or occupational movement restrictions that aggravate the presenting condition | Supports active care frequency and validates why passive home-based recovery is clinically inadequate |
| Z59 | Problems related to housing and economic circumstances | Patient identifies housing instability, overcrowding, or documented economic hardship affecting treatment access or recovery environment | Establishes why the patient's living conditions extend the clinically necessary care timeline beyond standard recovery benchmarks |
| Z59 (transportation subset) | Lack of adequate transportation | Patient lacks reliable transport to access alternative care settings or maintain consistent home therapy protocols | Directly validates in-office active care with frequent adjustments as the clinically supported decision over home-based options |
| Z60 | Problems related to social environment | Patient presents with social isolation, limited support network, or documented adjustment difficulties affecting treatment compliance | Explains deviation from expected recovery timeline and supports the care frequency documented in the active care plan |
| Z63 | Other problems related to primary support group and family circumstances | Patient identifies household stressors, caregiver burden, or family conflict contributing to chronic musculoskeletal presentation | Provides codified documentation that psychosocial and environmental factors are driving the complexity of the clinical picture |
How to Document SDOH Codes Without Slowing Down Your Front Desk
Knowing the codes is the easy part.
The breakdown happens at the front desk — where a team already managing check-ins, phone calls, and insurance verifications gets handed a new documentation requirement with no workflow behind it.
It doesn't fail because clinicians push back.
It fails because nobody built it into intake. When the process is undefined, the codes get skipped. And skipped codes mean undefended files.
The fix isn't complex. It's structural.
A short screening form — embedded into intake paperwork you're already using — captures SDOH data before the patient reaches the table. The clinician verifies. The record gets updated. The file is defended.
That sequence doesn't slow down your front desk. But it has to be built on purpose.
Who on Your Team Can Collect SDOH Data — and What CMS Requires
CMS finalized guidelines permitting any member of the healthcare team to collect SDOH data — including front-desk staff and clinical support personnel.
The requirement is not that a clinician conduct the screening. The requirement is that a clinician verifies the information and that it is documented in the patient's medical record.
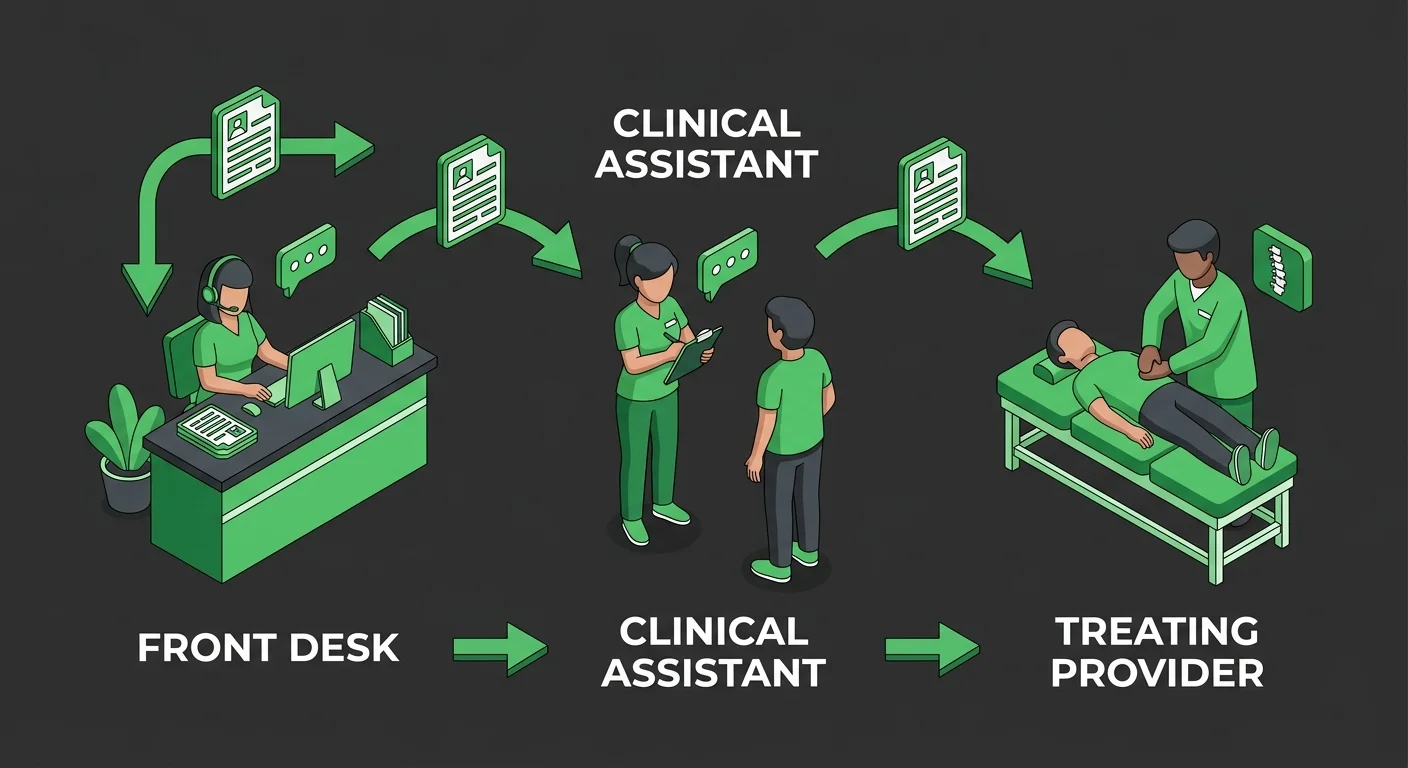
Here's what that looks like in practice.
A front-desk coordinator hands a patient a one-page screening form at intake. The patient fills it out. The coordinator enters the responses. The treating chiropractor reviews and signs off at the point of care.
That's the entire workflow — and it fully satisfies CMS documentation requirements.
CMS doesn't just review individual claims. It tracks Z-code frequency patterns across clinics — and uses that data to assess audit risk.
Practices where staff collect SDOH data and clinicians verify it produce a consistent, recurring documentation pattern. That's what CMS quality metrics reward.
Practices that skip this step produce the exact gap those same metrics flag. The difference isn't clinical capacity. It's whether the process exists at all.
The Documentation Workflow That Protects Your Practice at Audit
The audit-proof workflow isn't complicated. But the sequence matters.
Screening happens at intake. Barriers get identified. The clinician ties those barriers directly to the clinical rationale in the visit note. The codes go in.
Now the file has a structural argument — not just a claim.
Transportation barriers are the clearest example of where this pays off.
When a patient doesn't have reliable transportation, in-office care with frequent adjustments is clinically necessary — not a preference. But that fact isn't self-evident to an auditor reading a claim.
When it's documented — coded under Z59, verified by the clinician, referenced in the visit note — the record makes the argument on its own. The distinction becomes defensible at the point of active care and maintenance documentation.
Practices that build this workflow now are the ones whose files will hold under 2026 audit pressure.
Not because they documented more. Because they documented the right things — in the right sequence — with clinician verification attached.
That's what an audit-proof file actually looks like. Not a longer chart note. A structurally complete argument, built from intake forward.
| Documentation Step | Who Completes It | CMS Requirement | Audit Protection Level |
|---|---|---|---|
| Patient intake screening form distributed | Front-desk coordinator or clinical support staff | CMS permits any healthcare team member to collect SDOH data | Foundational — captures barrier data before the visit begins |
| Patient completes SDOH screening form | Patient (self-report during check-in) | Data must be documented in the patient's medical record | Baseline — creates a patient-generated record of identified barriers |
| Coordinator enters responses into patient record | Front-desk coordinator or clinical support staff | Documentation must appear in the official medical record | Structural — places barrier data in the defensible file before the adjustment |
| Clinician reviews and verifies documented SDOH data | Treating chiropractor | Practitioner verification is required by CMS | Critical — clinician sign-off converts collected data into a compliant, audit-ready record |
| Clinician ties identified barriers to clinical rationale in visit note | Treating chiropractor | Barrier documentation must support the clinical decision recorded | Highest — connects SDOH code directly to the medical necessity argument in the file |
| Z-code entered on the claim alongside primary diagnosis | Billing staff or embedded billing partner | Z-codes must align with documented clinical record entries | Complete — transforms a coded barrier into a structural argument that stands under audit review |
Frequently Asked Questions
But commitment requires clarity. Here are the questions practices actually ask before they change anything.
Most of the confusion isn't about the codes themselves. It's about what the codes actually require the practice to do.
What are the new 2026 ICD-10 SDOH codes for chiropractors?
The relevant blocks sit within the Z55–Z65 range. Z59 covers housing instability and economic barriers. Z60 addresses social isolation and environment. Z63 captures family relationship stressors. Z56 documents occupational and employment barriers. Transportation limitations are also coded within Z59.
The CDC's NCHS maintains the Z55–Z65 blocks as the official classification system for socioeconomic factors affecting clinical outcomes. None of these require a formal medical diagnosis. They require documented observation — a barrier identified, entered in the record, and verified by the treating clinician.
Why is Medicare auditing chiropractic SDOH code documentation?
CMS structural programs actively evaluate Z-code frequency to assess clinic-level audit risk. Historically, fewer than 2% of chiropractic encounters utilized SDOH codes. That gap is visible in CMS quality metrics.
CMS is not auditing because practices overuse these codes. It is auditing because missing environmental context creates unexplained care frequency. Unexplained care frequency is exactly what triggers review.
The documentation gap is the signal — not a missing diagnosis code.
Does a chiropractor need a formal diagnosis to bill a Z-code?
No diagnosis required. Z-codes document socioeconomic and environmental factors — not clinical conditions.
What's required is documented observation. A barrier identified, entered in the patient's record, and verified by the treating clinician. A patient who reports transportation barriers doesn't need a separate diagnosis. That barrier, documented and signed off by the chiropractor, is sufficient.
The threshold is consistency — not clinical complexity.
How do SDOH Z-codes affect clinical reimbursement rates?
SDOH Z-codes are non-payable. They don't add a revenue line. That's not what they're for.
They protect the revenue already in the claim. They build the structural argument for why the care plan required what it required. When a payer questions care frequency, the practice with documented housing instability or transportation barriers has a codified answer sitting in the record.
The practice without that documentation doesn't. That gap is where revenue disappears at audit — not at submission.
Can chiropractic office staff document social determinants of health?
Yes. CMS finalized guidelines permitting any member of the healthcare team to collect SDOH data — including front-desk staff and clinical support personnel. The clinician doesn't conduct the screening. The clinician verifies it and confirms it's documented in the patient's medical record.
Here's what that looks like in practice: a front-desk coordinator administers the intake form, the patient responds, the coordinator enters the data, and the treating chiropractor reviews and signs off at the point of care.
That sequence fully satisfies CMS documentation requirements. No clinical complexity required — just a consistent workflow.
Z-Codes Are Load-Bearing Walls — Build Them Into Your Billing Now
A Z-code is not a revenue line — it is a structural argument. That is the whole distinction. Practices treating SDOH codes as optional overhead aren't just skipping codes. They're pulling out load-bearing walls. The file looks complete from the outside. Under audit pressure, it collapses — because there's no codified explanation for why the care plan required what it required.
The practices that survive 2026 audit scrutiny won't be the ones that submitted the most claims — they'll be the ones that built the most defensible files. Transportation barriers documented. Housing instability coded. Occupational demands entered and clinician-verified. That sequence transforms a billing file from a claim into an argument. And an argument built from intake forward is one that stands on its own when a payer questions care frequency, duration, or necessity.
Bushido Billing builds this layer in from the start — because documentation that protects revenue is documentation that was constructed deliberately, not assembled after the fact. The Z-codes exist. The CMS framework is in place. The workflow is achievable. The only question left is whether your practice builds these structural arguments now — or explains their absence when the audit arrives.
CMS built the framework. The Z-codes are live. A Z-code is not a revenue line — it is a structural argument. The only question is whether your documentation is built to make that argument — or built to hope an auditor never asks.
Book a Call to see how your documentation holds up under audit pressure

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet