

How to Update Your Chiropractic Fee Schedule to Reflect 2026 Medicare Conversion Factor Cuts?
A fee schedule is not a price list. It is a compliance document.
Updating your chiropractic fee schedule for 2026 is not a math problem. It is a compliance problem that happens to involve math.
The Medicare Physician Fee Schedule controls pricing across more than 10,000 billing codes. When CMS finalizes a new conversion factor — as it did for CY 2025 at $32.35, a 2.83% decrease from the prior year — every code on the schedule recalculates. Practices that treat this as a simple percentage adjustment are solving for the wrong thing.
The real exposure is not the rate change. It is what happens to claims when the clinical documentation behind them cannot defend the codes being billed.
Medicare chiropractic coverage is strictly limited to manual manipulation of the spine to correct a subluxation, as defined in the Medicare Benefit Policy Manual, Chapter 15, Section 240. That boundary is narrow. Any claim that strays outside it — or fails to signal active treatment correctly — is denied before the rate ever becomes relevant.
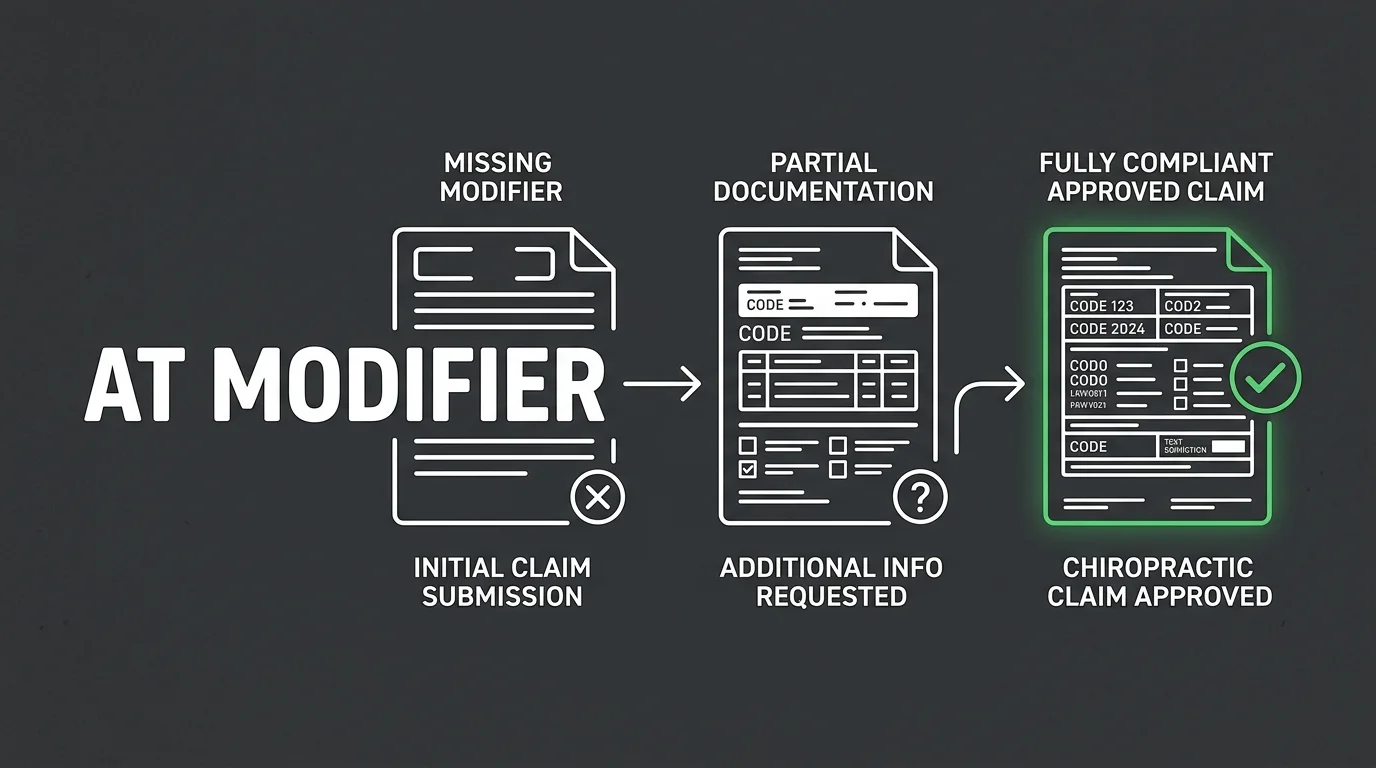
The AT modifier is the mechanism that separates active care from maintenance care on a Medicare claim. A chiropractic Medicare claim submitted without it is automatically designated as maintenance care and denied 100% of the time. No modifier. No payment. The conversion factor is irrelevant if the claim never pays.
Updating a fee schedule correctly in 2026 means running five sequential steps: retrieve the regional conversion factor, audit active care documentation, map AT modifier compliance across all active codes, reconcile the fee schedule against regional maximums, and validate the result with a human billing review. Skipping any one of them leaves a gap the rate change exposes.
Every number on your fee schedule is only as defensible as the clinical documentation behind it. That is what this update is actually about.
Last Updated: June 22, 2026
- • What the 2026 Medicare Conversion Factor Cut Actually Means for Chiropractic Revenue
- • Why a Fee Schedule Is a Compliance Document, Not a Price List
- • The Step-by-Step Fee Schedule Update Process for 2026
- • AT Modifier Compliance: The Non-Negotiable Coding Rule That Protects Every Claim
-
• Frequently Asked Questions About Updating Your Chiropractic Fee Schedule for 2026
- • How do the 2026 Medicare conversion factor cuts directly impact my chiropractic fee schedule?
- • What are the most common mistakes chiropractic practices make when scaling fee schedules using automated EHR tools?
- • How does AT modifier compliance protect our practice against Medicare conversion factor decreases?
- • What steps should a chiropractic clinic take to audit and update active care documentation for 2026?
- • Can a chiropractic practice charge Medicare patients differently from standard cash-pay fee schedule rates?
- • What a Fee Schedule Update Actually Buys Your Practice in 2026
What the 2026 Medicare Conversion Factor Cut Actually Means for Chiropractic Revenue
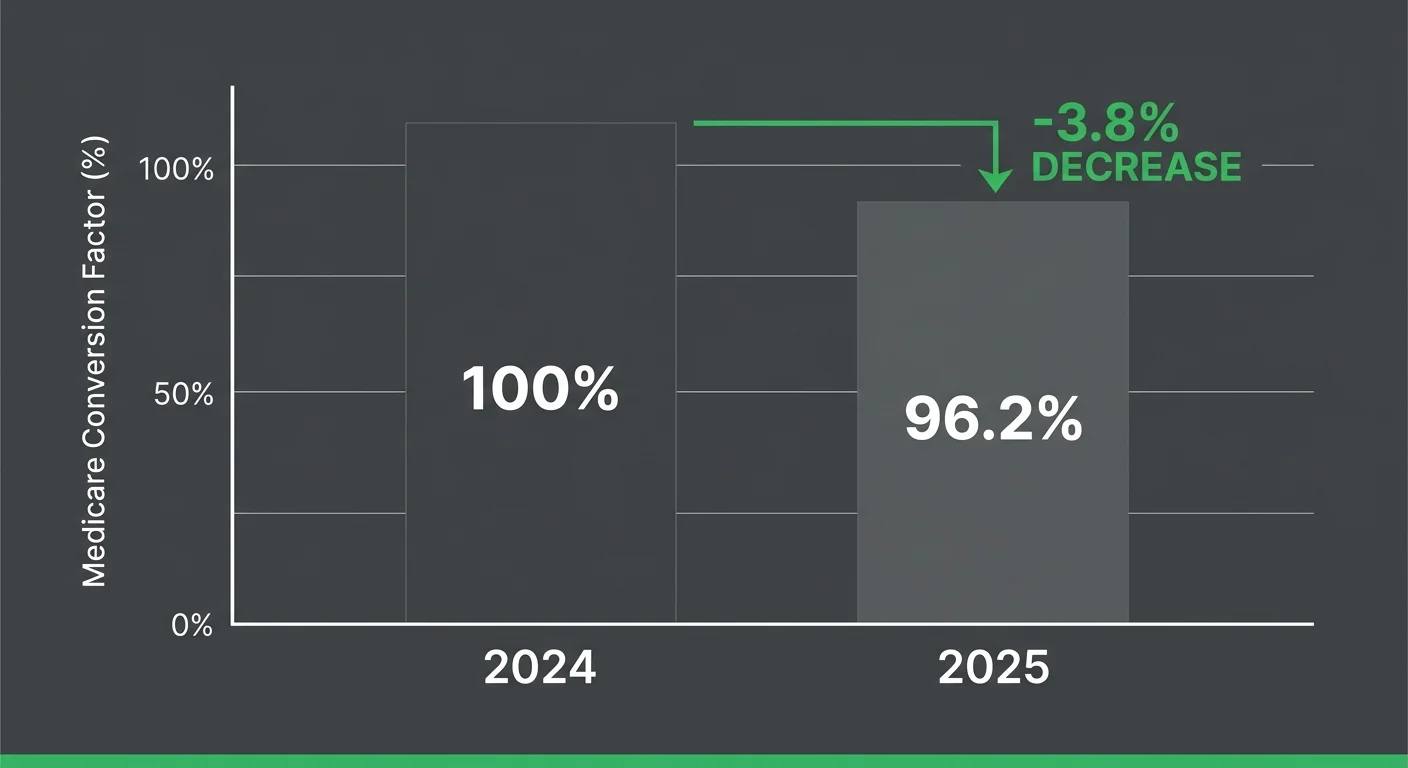
The CY 2025 conversion factor landed at $32.35 — a 2.83% decrease from the prior year — and 2026 is tracking the same direction.
That percentage sounds small. Run it across every Medicare claim a chiropractic practice submits in a year, and it stops sounding small.
The Medicare Physician Fee Schedule controls pricing across more than 10,000 billing codes. It's not a chiropractic document — but chiropractic practices feel every conversion factor move more acutely than most specialties do. That's not a coincidence. It's a function of how narrow the covered scope actually is.
The MACRA payment framework enacted in 2015 set the long-term update parameters that still drive how CMS calculates each year's conversion factor. These annual cuts aren't accidents or oversights. They're baked into the formula.
The practices absorbing the most damage are the ones treating each cut as a standalone math problem — update the number, move on. That response misses the real threat entirely.
How the Conversion Factor Translates Into Per-Claim Revenue Loss
Here's the mechanism most practices skip over.
The conversion factor is a multiplier applied to each code's relative value unit. When the multiplier drops, every code's reimbursement drops with it — proportionally, all at once.
A 2.83% decrease looks like a rounding error on a single claim. Run it across dozens of Medicare chiropractic claims per week for a full year, and it becomes a material revenue gap — not a footnote.
That gap gets worse when the fee schedule hasn't been updated to reflect current regional maximums. Practices that undercharge relative to the allowable are leaving money on the table regardless of what the conversion factor did. The cut and the stale schedule compound each other.
The deeper problem isn't the adjustment — it's the silence around it. A fee schedule that doesn't reflect the correct conversion factor creates a mismatch between billed charges and allowable reimbursement. That mismatch shows up as underpayments, not denials. Nobody flags them. Nobody works them.
They sit until someone audits the books. By then, the recovery window is usually closed. Practices that want the full picture of what 2026 regulatory exposure actually costs them need to understand the 2026 regulatory defense strategy.
Why the Cut Hits Chiropractic Harder Than Other Specialties
Chiropractic's exposure is structurally different from every other specialty on the fee schedule.
Most specialties bill across dozens of procedure codes and service categories. Chiropractic Medicare billing is concentrated — covered scope is limited to spinal manipulation for active subluxation correction, and the codes carrying that work are few.
That concentration means the cut hits a narrower revenue base harder. There's no spread across procedure types to cushion the loss.
For most specialties, one code is a fraction of total revenue. For a chiropractic practice, the majority of Medicare revenue can run through a small handful of spinal manipulation codes — all subject to the same multiplier drop at the same time. The revenue cycle management work a billing partner does in that context isn't administrative overhead. It's defense.
And then there's the AT modifier — which makes all of this worse.
Chiropractic Medicare claims must signal active care to be payable at all. The AT modifier isn't an optional code enhancement. It's the gate the claim has to pass through before the conversion factor even applies. No modifier, no payment — the conversion factor is irrelevant.
A practice absorbing a 2.83% rate cut while also losing claims to AT modifier errors isn't dealing with one problem. It's dealing with two that compound each other.
| Metric | CY 2024 Baseline | CY 2025 Rate | Impact on Chiropractic Claims |
|---|---|---|---|
| Medicare Physician Fee Schedule Conversion Factor | Above $32.35 (prior year baseline) | $32.35 | Every chiropractic spinal manipulation code reimbursement recalculates downward proportionally |
| Year-over-year conversion factor change | Prior year rate (CY 2024 baseline) | 2.83% decrease | Compounding annual revenue gap across all Medicare chiropractic claims submitted per week |
| Billing codes governed by MPFS | Over 10,000 codes across all specialties | Over 10,000 codes — same scope | Chiropractic revenue is concentrated in a narrow set of spinal manipulation codes — the cut hits a smaller revenue base harder |
| Legislative framework driving annual update parameters | MACRA (2015) parameters in effect | MACRA parameters continue to govern CY 2025 and forward | Annual cuts are structurally predictable — not isolated events — making fee schedule updates a recurring compliance requirement, not a one-time correction |
Why a Fee Schedule Is a Compliance Document, Not a Price List
Most practices treat the fee schedule like a rate card. Update the number, move on. That's exactly why the annual update keeps failing them.
Here's the thing: every number on a fee schedule is only as defensible as the clinical documentation behind it. If the documentation can't support the code being billed, the rate is irrelevant. The claim doesn't pay — regardless of what the schedule says.
That's the reframe. The fee schedule update is a documentation audit first. The math comes second.
What Medicare Actually Covers for Chiropractic — and What It Doesn't
Medicare's coverage window for chiropractic is narrower than most practitioners realize. Published policy guidance spells it out without ambiguity: Medicare Benefit Policy Manual Chapter 15 Section 240 limits chiropractic coverage strictly to manual manipulation of the spine to correct a subluxation. Not spinal therapy. Not adjunctive services. Manual manipulation — for active subluxation correction — and nothing else.
That boundary doesn't flex. Services outside it don't get reimbursed. And claims inside it that fail to signal active care correctly get denied just as completely.
So the AT modifier isn't an administrative detail. It's structural. Yes, clinicians need to update their fee schedules annually to avoid billing below the regional Medicare maximum allowable charge — but that update is worthless if claims can't clear the active-care gate first. The fee schedule and the documentation behind it are one system. You don't get to fix one without the other.
Why Simple EHR Rate Scaling Fails Chiropractic Practices
EHR platforms are built to submit claims. They're not built to defend them. When a practice runs automated rate-scaling to update the fee schedule, the software recalculates numbers. It doesn't audit whether the clinical documentation behind each code can support the updated rate under Medicare's coverage rules. Those are two completely different jobs.
The AT modifier is the clearest proof of that gap. A Medicare chiropractic claim submitted without it gets automatically designated as maintenance care and denied 100% of the time. No EHR rate-scaling tool catches that. No automated percentage adjustment prevents it.
Published research on denial patterns makes the consequence plain: the denial rate for non-AT-modified maintenance care claims is total. That's not a compliance edge case. It's a structural billing failure — and a fee schedule update, by itself, does nothing about it. Practices that scale rates without auditing modifier compliance are updating their price list while leaving the real exposure completely untouched.
What catches this is a human billing review. Automated tools process what they're programmed to process — and AT modifier compliance requires clinical judgment, documentation review, and a real understanding of how active care is being recorded at the visit level. No software does that. For practices building a full picture of their 2026 exposure, the 2026 ICD-10 and Medicare regulatory defense strategy puts this modifier risk inside the broader compliance framework where it belongs.
| Fee Schedule Element | What Most Practices Do | What Medicare Actually Requires | Consequence of the Gap |
|---|---|---|---|
| Procedure code selection | Choose the code that reflects the service performed and apply the updated rate | Code must align with documented clinical necessity for active subluxation correction — not just service type | Claim billed at the correct rate but denied for insufficient medical necessity documentation |
| AT modifier application | Apply the modifier by default or rely on EHR to populate it automatically | Modifier must reflect a clinician-level determination that the visit constitutes active, medically necessary care — not maintenance | Claims flagged as maintenance care are denied in full regardless of rate accuracy |
| Annual rate update | Scale existing fees by a percentage to match the new conversion factor | Rate update must be accompanied by a documentation audit confirming each code's clinical support still holds under current Medicare coverage rules | Updated rates sit on top of undocumented or misclassified services — the math is correct, the claim still fails |
| Coverage scope boundary | Bill all services rendered that relate to the patient's spinal condition | Medicare chiropractic coverage is limited to manual manipulation of the spine for active subluxation correction — adjunctive and maintenance services are excluded | Non-covered services submitted for reimbursement generate denials that erode both revenue and payer standing |
| Fee schedule validation | Confirm the updated schedule matches the published conversion factor and regional allowable | Validate that every billed code is supported by visit-level documentation that would survive a medical necessity review | Underpayments and denials accumulate invisibly until an audit surfaces the gap — often past the recovery window |
The Step-by-Step Fee Schedule Update Process for 2026

So here's what fixing it actually looks like.
Five steps — and they run in order. Skip one and you don't leave a gap. You break the integrity of everything that follows.
Step 1: Retrieve Your Regional Conversion Factor
Start with the CMS Physician Fee Schedule lookup tool. Pull the conversion factor for your specific Medicare Administrative Contractor (MAC) region. Not the national average. Not last year's number.
Regional variation is real. The allowable reimbursement for a given spinal manipulation code differs by locality. A practice billing to a national figure instead of its regional maximum is already leaving recoverable revenue on the table — and the conversion factor cut hasn't even entered the picture yet.
The CY 2025 conversion factor finalized at $32.35 — a 2.83% decrease from CY 2024. For 2026, the directional trend is the same. Pull your confirmed regional figure, record it, and treat it as the fixed baseline for every calculation that follows.
Step 2: Audit Active Care Documentation
Here's what most practices skip: before any rate gets recalculated, the documentation behind every active code has to hold up on its own.
Medicare coverage for chiropractic is strictly limited to manual manipulation of the spine to correct a subluxation — per the Medicare Benefit Policy Manual, Chapter 15, Section 240. That boundary doesn't flex. If the clinical documentation doesn't clearly establish active subluxation and medical necessity, the code isn't payable. Not at the updated rate. Not at any rate.
Pull the documentation for every code currently on the fee schedule. Confirm that each active-care designation is supported by visit-level clinical notes. Documentation gaps discovered here don't get fixed by updating the math. They get fixed by fixing the documentation.
Step 3: Map AT Modifier Compliance Across All Codes
Most fee schedule updates never get here. That's exactly why most fee schedule updates don't work.
Go code by code. For every Medicare chiropractic spinal manipulation code on the schedule, confirm the AT modifier is applied correctly and that visit-level documentation supports active care — not maintenance. A claim submitted without the AT modifier on a Medicare chiropractic service isn't a recoverable denial. It is a structural billing failure that repeats on every future claim until the compliance gap is closed.
This is also the right moment to run a structured internal chiropractic coding audit before the 2026 changes take effect.
Step 4: Reconcile Fee Schedule Against Regional Maximums
Documentation confirmed. Modifier compliance mapped. Now the rate math actually means something.
Apply the updated regional conversion factor to each code's relative value units. Then compare every recalculated charge against the regional Medicare maximum allowable. The goal isn't just a proportional adjustment from last year's number — it's confirming each new rate sits correctly above the regional floor. Clinicians must update fee schedules annually to prevent billing below that regional maximum. This step is how you verify the update actually accomplished that.
Any code where the billed charge falls below the regional allowable is a recoverable gap. Document each discrepancy. This reconciliation is what Steps 1 through 3 produce when they've been run in order. Run them out of order — or skip one — and the numbers here can't be trusted.
Step 5: Validate With a Human Billing Review
A human billing review isn't a final quality check. It's what holds the entire process together.
Automated tools recalculate rates. That's the full extent of what they do. They don't assess whether the documentation behind a code can survive Medicare scrutiny. They don't evaluate whether AT modifier usage is clinically consistent across visit types. They don't catch reconciliation discrepancies that only surface when someone reads the notes. That requires judgment. Software doesn't have it.
A billing professional who understands chiropractic documentation standards and the Medicare coverage window — the strict spinal manipulation limit under Chapter 15, Section 240 — is the last line of review before the updated schedule goes live. The practices that protect revenue in 2026 are the ones who treated this as a documentation audit first. The math was always the easy part.
| Step | Action Required | Who Is Responsible | Common Failure Mode | Completion Signal |
|---|---|---|---|---|
| Step 1 — Retrieve Your Regional Conversion Factor | Pull the confirmed conversion factor for your specific Medicare Administrative Contractor (MAC) region from the CMS Physician Fee Schedule lookup tool | Billing team or embedded billing partner | Using the national average or prior year's figure instead of the current regional rate | Regional conversion factor documented and confirmed as the baseline for all subsequent calculations |
| Step 2 — Audit Active Care Documentation | Review clinical notes behind every active code on the fee schedule; confirm each active-care designation is supported at the visit level | Provider and billing reviewer working together | Skipping documentation review entirely and proceeding directly to rate recalculation | Every active code has confirmed visit-level documentation establishing medical necessity for spinal manipulation |
| Step 3 — Map AT Modifier Compliance Across All Codes | Go code by code through all Medicare chiropractic spinal manipulation codes; verify AT modifier is applied and clinical documentation supports active — not maintenance — care | Human billing reviewer with chiropractic Medicare expertise | Assuming modifier compliance is correct without a dedicated code-level review | Every Medicare manipulation code on the schedule has documented AT modifier alignment before rates go live |
| Step 4 — Reconcile Fee Schedule Against Regional Maximums | Apply the updated regional conversion factor to each code's relative value units; compare every recalculated charge against the regional Medicare maximum allowable | Billing team | Adjusting rates proportionally from the prior year without confirming position relative to the regional floor | All billed charges documented as correctly positioned above the regional maximum allowable with discrepancies flagged and resolved |
| Step 5 — Validate With a Human Billing Review | Have a billing professional review the full updated schedule for documentation defensibility, modifier consistency, and reconciliation accuracy before the schedule goes live | Embedded billing partner or senior billing reviewer | Treating this step as optional or replacing it with a software audit | Updated fee schedule signed off by a qualified human reviewer and cleared for implementation |
AT Modifier Compliance: The Non-Negotiable Coding Rule That Protects Every Claim
But inside that five-step process, one coding rule overrides everything else. The AT modifier is what determines whether a Medicare chiropractic claim gets paid or denied on first submission — nothing else comes close.
Every other step in the fee schedule update builds toward this point. Pull the regional conversion factor. Audit documentation. Reconcile rates against regional maximums. None of that work converts to revenue if the AT modifier is missing or misapplied. The claim is denied before the rate ever enters the picture.
And it's not a modifier you set once at the start of a calendar year. It requires active clinical documentation at the visit level, consistent application across every eligible claim, and a billing process that catches gaps before submission — not after the denial arrives.
What the AT Modifier Does — and When It Must Appear
The AT modifier sends one signal to Medicare: this patient is receiving active treatment, not maintenance care. That distinction matters because Medicare coverage for chiropractic is narrow by design. Under the Medicare Benefit Policy Manual, Chapter 15, Section 240, coverage is strictly limited to manual manipulation of the spine to correct a subluxation. The AT modifier is how a claim declares that the service being billed falls inside that window.
Without it, Medicare reads the claim differently. A chiropractic manipulation submitted without the AT modifier is automatically classified as maintenance care. Maintenance care is not a covered benefit. The claim doesn't get reduced. It gets denied entirely.
The modifier belongs on every spinal manipulation code billed to Medicare where active care applies. It's not a practice-level setting. It's a claim-level declaration — and it has to be backed by visit-level documentation that establishes medical necessity, identifies the subluxation being treated, and reflects active improvement or the expectation of it. That's the coverage boundary Chapter 15, Section 240 draws. The documentation behind each claim either clears that line or it doesn't. Practices working through this documentation standard will recognize the same logic at work in visit-level documentation interacts with add-on codes.
The Denial Pattern That Emerges When AT Modifier Documentation Breaks Down
The denial pattern that follows AT modifier gaps is predictable. A practice with inconsistent documentation doesn't see random denials scattered across the claim set. It sees denials clustered around specific visit types, specific providers, or specific periods when documentation standards slipped.
Chiropractic Medicare claims without the AT modifier are denied 100% of the time. That is not a worst-case figure. It is the structural outcome of the rule. There is no partial payment, no reduced allowable, and no appeal pathway that converts a maintenance-care designation into an active-care reimbursement.
What compounds the damage is the lag. Practices rarely find modifier gaps through real-time claim tracking. They find them in an AR aging report that shows a pattern of denials nobody worked. By then, the documentation window for the affected claims may have closed, the appeals timeline has passed, and the revenue is gone. Proactive weekly communication between a billing partner and the practice is what surfaces these patterns before they age past the point of return.
And a fee schedule update doesn't close this gap. Scaling rates by the new conversion factor — manually or through an EHR software tool — recalculates what the practice intends to charge. It does not audit whether the modifier compliance supporting each claim is intact. The math and the documentation are separate systems. Treating them as one is where practices lose revenue they should have protected.
Who Should Not Be Billing Chiropractic Claims Without Specialty Oversight
Here's the behavior worth naming directly. Some practices bill chiropractic Medicare claims using generalist billing staff or generic medical billing services that don't carry specialty-level knowledge of chiropractic coding rules. That is not a comment on effort. It is a structural problem with real consequences.
The AT modifier is not a universal billing concept. It's a chiropractic-specific Medicare rule — one that requires understanding the coverage boundary under Chapter 15, Section 240, how active care is documented at the visit level, and how maintenance-care designations cascade across a claim set when documentation is inconsistent. A generalist biller processing chiropractic claims does not carry that knowledge by default. The result is the same as having no modifier compliance at all: a 100% denial rate on affected claims.
Here's the test. If the billing operation handling chiropractic Medicare claims can't explain the AT modifier requirement without being asked — or can't show where in the documentation workflow active care is confirmed before submission — that is the answer. A fee schedule is only as defensible as the specialty knowledge behind it.
| Claim Scenario | AT Modifier Present | Documentation Standard Met | Medicare Payment Outcome |
|---|---|---|---|
| Spinal manipulation billed to Medicare — active care, AT modifier present, documentation supports subluxation and active improvement | Yes | Yes | Claim processes for payment under Medicare Physician Fee Schedule allowable |
| Spinal manipulation billed to Medicare — AT modifier missing, visit notes do not establish active care | No | No | Claim auto-classified as maintenance care — denied 100% of the time, no partial payment, no appeal pathway to active-care reimbursement |
| Spinal manipulation billed to Medicare — AT modifier present, but visit-level notes reflect maintenance pattern without active improvement | Yes | No | Claim subject to post-payment audit and retroactive denial; modifier present but unsupported documentation creates recoupment exposure |
| Spinal manipulation billed to Medicare — AT modifier present, documentation supports subluxation, but conversion factor not updated to CY 2025 regional allowable | Yes | Yes | Claim paid, but at under-billed rate — practice leaves recoverable revenue on the table due to stale fee schedule |
| Non-spinal service billed to Medicare under a chiropractic NPI — outside covered benefit scope, AT modifier not applicable | N/A | N/A | Claim denied — service falls outside the covered benefit boundary; AT modifier cannot override coverage exclusion |
Frequently Asked Questions About Updating Your Chiropractic Fee Schedule for 2026
Good. Now let's get to the questions practitioners actually ask.
Five questions. Straight answers. No qualifications.
How do the 2026 Medicare conversion factor cuts directly impact my chiropractic fee schedule?
The CY 2025 conversion factor was finalized at $32.35 — a 2.83% decrease from CY 2024. Every Medicare-paid code recalculates at a lower base rate. That's the starting point. But here's where practices actually lose money: a fee schedule that doesn't reflect the updated rate means you're billing below the regional maximum allowable. That's recoverable revenue you're leaving on the table — not because Medicare denied anything, but because your numbers were stale. The fee schedule is the foundation. Everything billed to Medicare flows through it.
What are the most common mistakes chiropractic practices make when scaling fee schedules using automated EHR tools?
Automated EHR tools recalculate rates. That's it. They don't assess whether your active-care documentation supports each code at the visit level. They don't check AT modifier consistency across your claims. They don't flag where your clinical notes would fail Medicare scrutiny. So what happens? The numbers update. The structural compliance gaps stay exactly where they were. The math changes. The denial pattern doesn't.
How does AT modifier compliance protect our practice against Medicare conversion factor decreases?
The AT modifier is the only signal Medicare accepts that a chiropractic claim represents active treatment. Without it, Medicare classifies the claim as maintenance care and denies it 100% of the time. Here's what that means in practice: a conversion factor cut reduces your reimbursement floor. Missing AT modifier compliance removes the floor entirely. Practices with consistent modifier documentation absorb a rate decrease. Practices without it absorb a 100% denial rate on affected claims — and it doesn't matter what rate you had on the fee schedule.
What steps should a chiropractic clinic take to audit and update active care documentation for 2026?
Start at the visit level. Pull a sample of Medicare claims from the past 90 days. For every encounter billed with the AT modifier, confirm that active-care documentation actually exists — subluxation identified, medical necessity established, active improvement recorded. Then check modifier consistency. Were there claims submitted without the AT modifier where active care applied? Cross-reference against your denial history. Clusters by visit type or provider are the signal. Documentation and modifier application have to be aligned before the updated fee schedule goes live. Updated rates on a broken documentation foundation don't protect you — they just make the denial math easier to calculate.
Can a chiropractic practice charge Medicare patients differently from standard cash-pay fee schedule rates?
Medicare sets the maximum allowable charge by region. You can't bill Medicare patients above that regional maximum. But you can — and should — bill at or up to it. Cash-pay patients aren't subject to Medicare fee schedule rules. Those schedules are separate. What they share is the documentation standard. Under Medicare Chapter 15, Section 240, coverage is strictly limited to manual spinal manipulation to correct a subluxation. That visit-level documentation requirement doesn't change based on how the patient pays — it applies regardless of payer. If your notes don't support the service billed, the payer mix doesn't save you.
What a Fee Schedule Update Actually Buys Your Practice in 2026
A fee schedule update done right buys one thing.
Defensibility.
Not a cleaner rate sheet. Not a better-looking spreadsheet. The ability to submit a Medicare chiropractic claim, have every element reviewed, and have every element hold — the regional conversion factor, the active-care designation, the AT modifier, the visit-level documentation behind it.
That's what the five-step process produces when it's worked in order. Steps 1 through 5 aren't independent tasks. They're a single compliance chain. Break it anywhere, and the rest of the work doesn't protect you.
The practices that struggle in 2026 won't struggle because the conversion factor cut was too steep.
They'll struggle because they treated a compliance overhaul like a math problem. They recalculated the rates. They didn't confirm AT modifier compliance across active codes. They didn't audit whether visit-level documentation could survive scrutiny. The updated numbers went live — and the same structural gaps that were generating denials before kept generating them after, now against a lower reimbursement floor.
Bushido Billing's position is direct: a billing operation that doesn't surface documentation gaps before submission isn't protecting your revenue. It's processing claims and hoping.
The practices that protect revenue in 2026 are the ones who understood what they were actually updating.
A fee schedule is not a price list. It is a compliance document — and every rate on it is only as defensible as the clinical documentation and modifier application behind it.
The math was always the easy part. What 2026 is testing is whether your billing operation treated the documentation audit as the real work — or skipped it entirely and called the numbers done.
That answer shows up in your AR.
Your fee schedule isn't a price list. It's a compliance document. And if the numbers you updated aren't backed by AT modifier discipline and visit-level documentation that holds up under scrutiny, you haven't protected your revenue — you've just changed the math on claims that still won't pay.

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet