

Bushido Billing vs. ChiroTouch Integrated Billing: Which Protects Your Revenue?
Integrated EHR billing protects your submission workflow. It does not protect your revenue.
ChiroTouch's integrated billing automates claim submission — but submission is not the same as revenue recovery, and the gap between the two is where chiropractic practices lose approximately 15% of their collectible income.
That's the distinction most comparison articles skip entirely. ChiroTouch's integrated billing platform is purpose-built for claim submission volume and automated throughput. When claims are clean — straightforward encounters with airtight documentation and simple payer mixes — it functions exactly as advertised. But the claims that threaten your revenue aren't clean. They're the complex, documentation-heavy, payer-specific denials that require human forensic work to recover. That's precisely where integrated automation reaches its structural ceiling.
According to Medicare Compliance Tips from CMS, the improper payment rate for chiropractic services sits at 33.6%, with 95.5% of those errors driven by documentation issues that automated systems are not designed to catch or correct. Software doesn't write clinical narratives. Software doesn't identify when a payer's local coverage determination has shifted and your documentation language needs to follow. A human does.
Bushido Billing operates as an embedded billing partner — not a software vendor. That means a dedicated biller working inside your existing ChiroTouch environment, forensic denial management on every high-friction claim, and weekly communication built into the operation as a structural feature. Not optional. Not a premium tier. The baseline.
This article compares both models across the dimensions that actually determine revenue outcome: incentive structure, denial recovery capability, ERA reconciliation, regulatory navigation, and what transparency looks like when something goes wrong.
If you're seeing green "Sent" checkmarks in your dashboard while your bank account tells a different story, this article explains exactly why — and what to do about it.
Last Updated: April 2026
- The Structural Difference Between Submission and Billing
- How Denial Management Actually Works — And Where Integration Breaks Down
- The Incentive Gap: Why Software Vendors and Billing Partners Want Different Outcomes
- Regulatory Navigation in 2026: Where Human Expertise Is Non-Negotiable
- FAQ
- Why does my ChiroTouch dashboard show claims as "Sent" when my collections aren't growing?
- What is the "Integrated Trap" in chiropractic billing?
- Does ChiroTouch's integrated service handle medical necessity appeals for Medicare?
- Is it more expensive to use an embedded billing partner than integrated billing?
- Can Bushido Billing work inside my existing ChiroTouch Cloud instance?
- When should I audit my current billing operation rather than just switching providers?
- What happens to my AR if I switch from integrated billing to Bushido?
- Conclusion: The Difference Between Submitting Claims and Getting Paid
The Structural Difference Between Submission and Billing
Every chiropractic practice running full-service chiropractic billing through a dedicated partner understands something integrated software users often don't: submission and billing aren't the same operation.
They look the same from the outside. Claim goes out. Status turns green. But what happens after that green light is where the two models diverge completely.
Submission is a mechanical step. Billing is everything that comes after — tracking the claim through adjudication, catching rejections before they age, reconciling payments to what was actually owed, and building the appeal when the answer comes back wrong. Software handles the first part. A billing partner handles all of it.
The industry defaults to treating submission as the finish line. It's the starting gun.
Why Integrated Billing Is Optimized for Volume, Not Recovery
Integrated billing is built for throughput. Claims leave fast, in volume, with minimal friction. For straightforward encounters where documentation is clean and payer adjudication is predictable, that's a real operational advantage.
The problem isn't what it does. It's what it stops doing after the claim goes out.
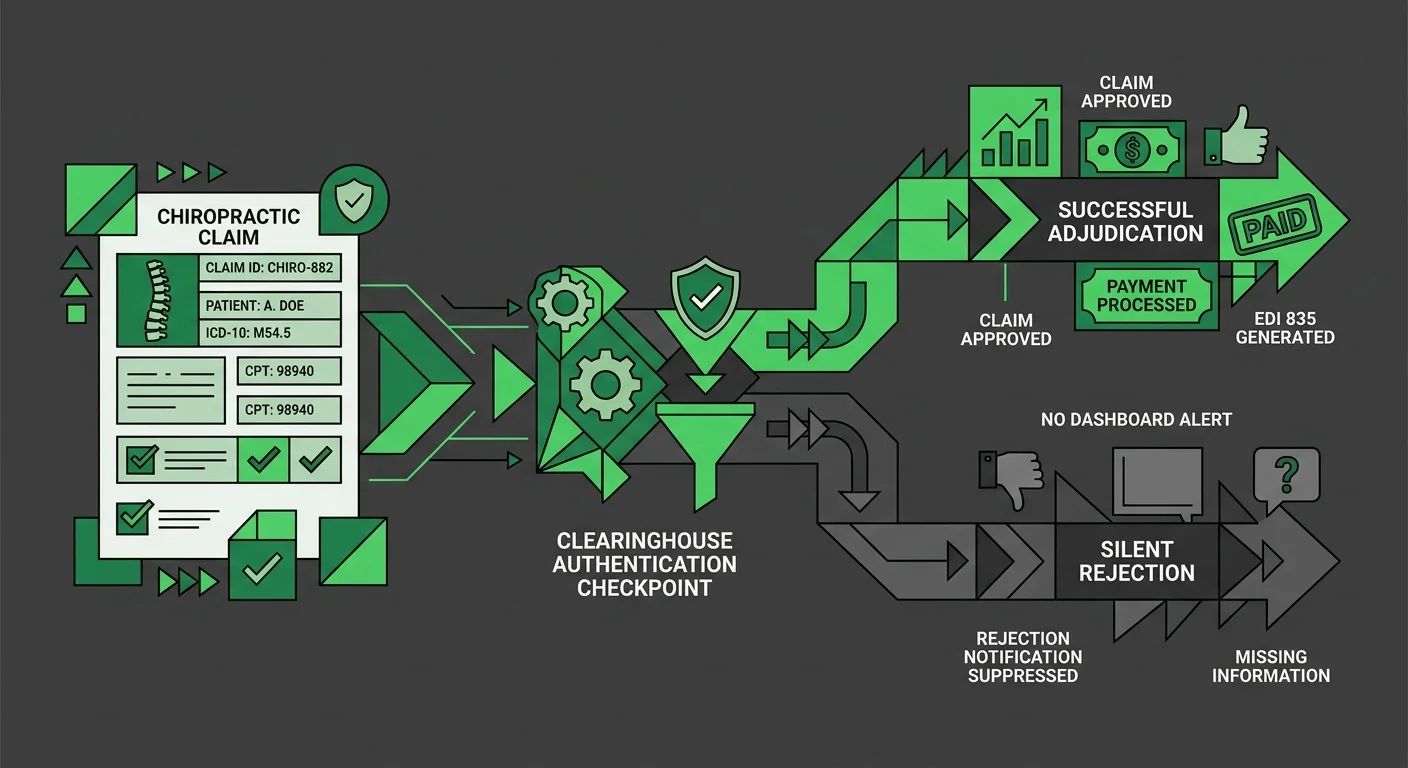
When a claim hits a clearinghouse authentication error, the software logs "Sent" — because the claim did leave your EHR. What it can't log is whether that claim was quietly rejected at the clearinghouse due to a credential mismatch, an EDI loop error, or a payer enrollment record that went stale after a software update. That failure doesn't produce a denial. It produces silence.
The MGMA EHR Transition Guide documents that EHR configuration changes frequently result in EDI and ERA connection gaps and elevated denial rates from misconfigured payer rules. That's not a software malfunction. It's the predictable outcome of any system that optimizes for submission speed over revenue accountability.
Nobody is watching what happens after "Sent." That's not a criticism — it's the boundary of what software can do. For practices dealing with the aftermath of a platform change, those gaps surface fast. Understanding ChiroTouch Cloud migration billing interruptions is usually the first diagnostic step when AR starts growing without a clear explanation.
The "Sent" Status Problem: What Your Dashboard Isn't Telling You
"Sent" means the claim left your software. That's all it means.
It doesn't mean the clearinghouse accepted it. It doesn't mean the payer received it. It definitely doesn't mean adjudication happened. A local status flag updated inside ChiroTouch — and then the claim went somewhere your dashboard can't follow.
Claims sit in a "Sent" state while silently failing at:
- Clearinghouse authentication — Payer enrollment credentials can desync after software updates or renewals, producing protocol-level rejections that never appear as denials in your system
- EDI loop validation — Structural formatting errors in the claim file trigger a clearinghouse rejection before the payer ever sees the claim, with no corresponding denial returned
- NPI or taxonomy mismatches — Configuration errors that pass internal EHR validation but fail payer-side processing entirely
- ERA orphaning — Payment posts but the ERA doesn't reconcile to the original claim; the revenue appears but the accounting never closes
Each of these requires a human who knows where in the chain to look. Automation can't investigate what it doesn't know is broken. Practices weighing the ChiroTouch Server vs. new billing partner decision in 2026 are often finding these gaps for the first time during the transition audit — and discovering they've been there for months.
| Claim Status | What It Confirms | What It Doesn't Confirm |
|---|---|---|
| Sent | Claim left your EHR software | Clearinghouse acceptance or rejection |
| Accepted | Clearinghouse validated format | Payer adjudication outcome |
| Denied | Payer rejected the claim | Whether the denial is appealable or already worked |
| Paid | Payment posted | Whether ERA reconciled correctly or ERA is orphaned |
How Denial Management Actually Works — And Where Integration Breaks Down
Every practice gets denials. That's not a billing failure — it's payer adjudication working as designed. Payers deny claims. The billing operation's job is to make sure those denials get worked.
What separates a practice with healthy collections from one with a growing 90-day AR bucket isn't the denial rate. It's what happens in the 30 days after a denial lands.
Medicare Compliance Tips from CMS shows that documentation deficiencies drive 95.5% of chiropractic improper payment findings. Most high-value denials aren't coding errors. They're documentation gaps — and closing them requires someone who can read the clinical record, understand what the payer's criteria require, and write a response that addresses both.
A workflow automation can flag the denial. It can't write that response.
The Volume-First Denial Model and What It Costs
Here's the standard denial workflow inside a volume-first model.
Denial arrives. System flags it. A batch review evaluates whether the claim is worth reworking. High-friction denials — those requiring documentation pulls, clinical narrative, multi-step appeals — get deprioritized. Cleaner claims that resubmit fast get worked instead.
That's not negligence. It's a rational operational decision for a business paid on submission volume, not collection outcome.
For your practice, it means the denials most likely to cost you the most money are exactly the ones least likely to get worked. They age. They compound. Eventually they fall outside the appeal window and become uncollectible.
The EHR Migration Risk Framework from Deloitte identifies financial reconciliation and internal controls as the most frequent failure points in integrated system implementations. The same pattern plays out in billing: when human review of denial patterns is absent, failures don't stop — they just stop being visible.
- Soft write-offs — Claims that never formally close but never get worked past the first denial
- Timely filing forfeitures — Appeals that miss the filing window because no one was tracking the 90-day clock per payer
- Underpayment acceptance — Payer pays below contracted rate; without ERA reconciliation, the shortfall posts as accepted and disappears into the numbers
- Duplicate denial patterns — The same documentation issue driving denials across dozens of claims for weeks before anyone connects the dots
Practices that went through a migration and are seeing these patterns should start with common data transfer errors in chiropractic EHR migrations — a significant share of what looks like billing failure traces back to how data transferred during the move.
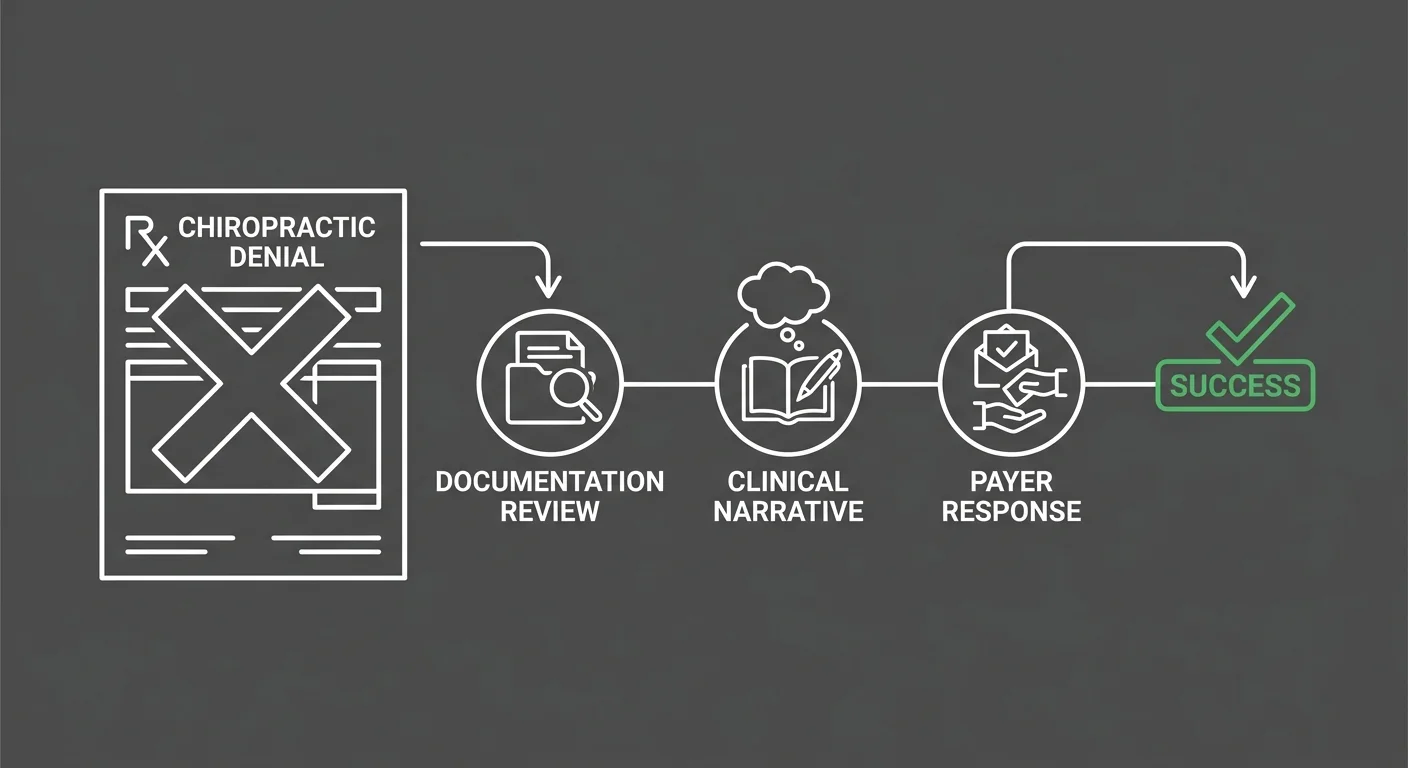
What Forensic Denial Management Actually Looks Like
Bushido's approach to denials starts before the claim goes out.
Pre-submission review. AT modifier verification. Subluxation documentation check against the clinical record. Payer-specific criteria reviewed before submission — not after adjudication returns a denial that could have been prevented.
For Medicare chiropractic claims, that means:
- AT modifier verification confirming active care documentation is complete before the claim leaves the system
- Subluxation documentation review ensuring the clinical record supports the diagnosis code as submitted
- Multi-step appeal architecture for medical necessity denials — not a generic redetermination, but a clinical narrative built around the patient's specific record and the payer's current criteria
When denials do come in, the weekly communication cadence means you know about pattern shifts the week they surface. Not when a quarterly AR review turns up a trend that's been building for 60 days. A payer changes a local coverage determination — you hear about it in your next weekly update. A wave of AT modifier rejections starts appearing — that's a conversation before it becomes a problem.
Denial spikes following a platform migration are especially common in the 60–90 day post-migration window. Payer enrollment mismatches, credential desyncs, and EDI configuration gaps all surface during that period — and none of them resolve on their own. For practices tracking this, ChiroTouch Cloud migration billing interruptions covers the specific failure modes to watch for.
| Denial Type | Integrated Billing Response | Embedded Partner Response |
|---|---|---|
| Medical necessity denial | Automated resubmission or write-off | Clinical narrative appeal with documentation review |
| AT modifier rejection | Flags for correction; may not catch root cause | Reviews documentation pattern across multiple claims |
| Timely filing denial | May miss if tracking is passive | Active 90-day clock monitoring per payer |
| ERA orphan | May post payment without reconciling | Human reconciliation closes every ERA to its claim |
| Underpayment | May post at payer's amount without audit | Contracted rate verification and dispute initiation |
The Incentive Gap: Why Software Vendors and Billing Partners Want Different Outcomes
Most comparison articles focus on features. This one focuses on incentives — because incentives explain what features can't.
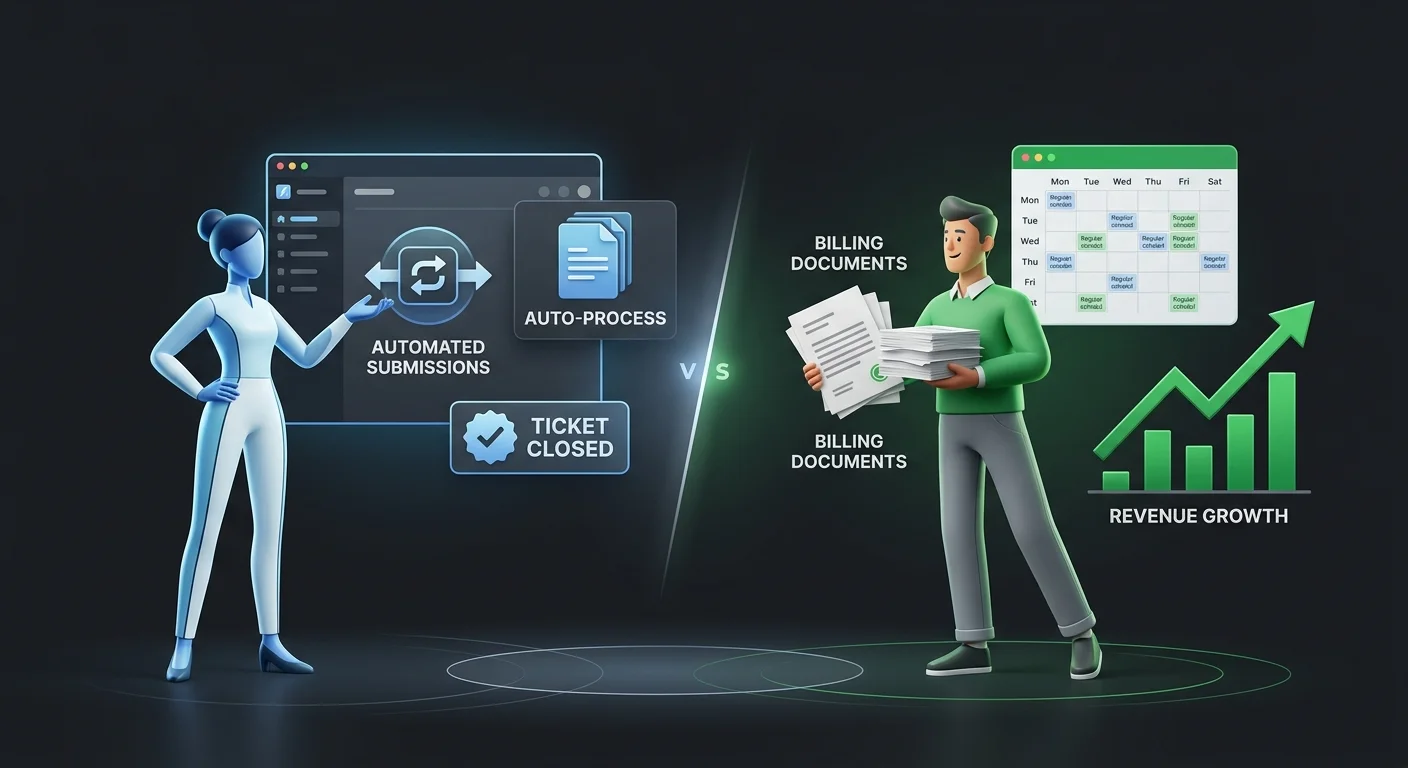
A software vendor gets paid when you renew. Support tickets close. Updates ship. The platform keeps running. Whether your AR is clean or quietly deteriorating has no bearing on that revenue relationship.
An embedded billing partner gets paid when you get paid.
That structural difference shapes everything downstream. It's why forensic denial management is standard practice here, not an upsell. It's why a dedicated biller is the base model. It's why weekly communication is built in — because a biller who isn't communicating proactively is one whose problems stay hidden until they've compounded into something harder to unwind.
Software vendors are incentivized to close tickets. Billing partners are incentivized to clear your AR.
Who This Is Not For
Worth being direct here.
If you're looking for the lowest billing rate, Bushido isn't the right fit. Performance-based billing is priced on recovery outcome. The practices that see the most value from it are the ones whose current model is leaving money on the table — not the ones optimizing for the smallest line item on a vendor comparison sheet.
If you want billing handled invisibly in the background with no communication and no involvement on your end, this isn't that model. The dedicated biller and weekly updates aren't optional. Transparency is structural here. A practice that doesn't want to see what's happening in their billing isn't who we work with.
If your integrated billing is genuinely working — clean payer mix, healthy AR, manageable denial rate — this article may not apply to you. The integrated model performs as intended for documentation-clean practices with simple payer profiles.
The practice this article is for is the one with green checkmarks in the dashboard and a growing 90-day AR bucket. The one whose current billing support can't give a specific answer about a specific claim. The one that's starting to wonder whether "Sent" means anything at all.
The Platform Agnosticism Advantage
The most common objection to switching billing partners is that it means switching software.
It doesn't.
Bushido works inside your existing ChiroTouch environment. Your billing software compatibility stays intact — ChiroTouch instance, clinical workflows, configuration, unchanged. What changes is the billing operation running inside it.
That's what also makes the embedded model well-suited for practices navigating the ChiroTouch Server-to-Cloud migration. The decision between staying on ChiroTouch Server or moving to a new billing partner doesn't require adding a software change on top of everything else. Bushido works in the system you're already on and handles the billing complexity migration introduces — without becoming another variable in an already disruptive transition.
Regulatory Navigation in 2026: Where Human Expertise Is Non-Negotiable
The 2026 chiropractic billing environment has more moving parts than it did two years ago. That's not alarmist framing — it's operational reality.
The EHR Modernization Report from Becker's and CSI Companies makes the point directly: platform modernization is an ongoing discipline, not a one-time implementation. Organizations that adopt unified platforms without proactive operational ownership create conditions where billing gaps emerge without visible warning. That's a precise description of integrated billing without a human watching the output.
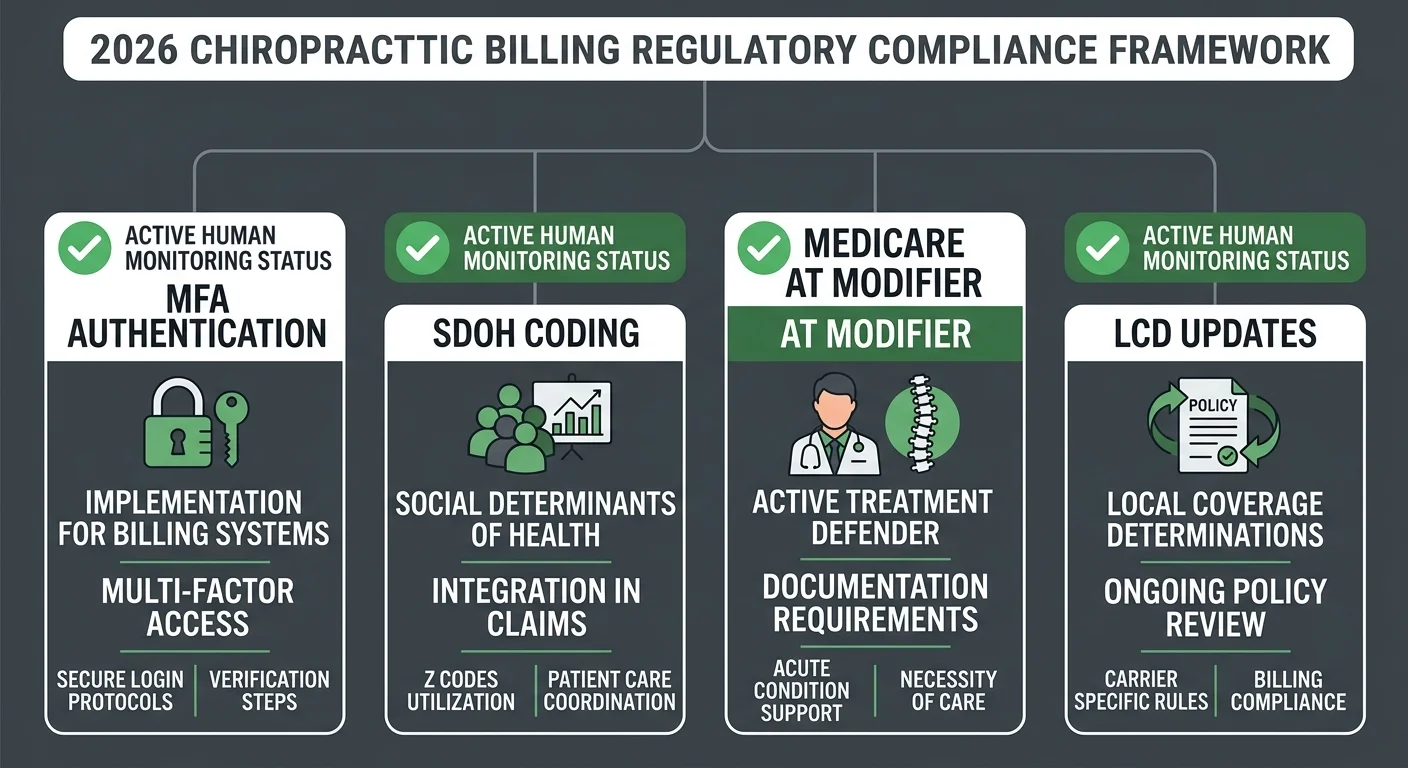
Three compliance pressure points are active for chiropractic practices right now:
- MFA and OAuth authentication requirements — Payer portal access increasingly requires multi-factor authentication tied to provider credentials. Post-migration credential desyncs are common and the failure mode is silent: claims stop reaching payers while the dashboard keeps showing "Sent"
- SDOH documentation requirements — Social determinants of health coding is expanding across payer contracts. Practices not actively tracking these requirements are building documentation gaps that surface as denials months after the encounters
- Medicare medical necessity documentation — The AT modifier requirement for active care isn't new. The scrutiny level is. Medicare Compliance Tips from CMS reflects a 33.6% improper payment rate — a number that format validation alone doesn't move
Why Automation Can't Navigate Regulatory Complexity
Software updates fee schedules. It adjusts claim formats when code sets change. That's genuinely valuable, and it's worth acknowledging plainly.
What it can't do is respond to a payer-specific LCD update that changed the clinical language required for medical necessity approval. It can't notice that a particular payer has shifted its adjudication pattern and that documentation needs to follow. It can't apply judgment to an edge case outside the rule set it was built against.
The EHR Migration Risk Framework from Deloitte identifies the reconciliation and control layer as the highest-frequency failure point in integrated system implementations — where automated processing meets the judgment required to catch what automation misses. Chiropractic billing in 2026 has exactly that failure point. Software handles the mechanical layer. A human handles everything the software can't.
When the human layer is absent, regulatory gaps don't announce themselves. They accumulate quietly until a pattern audit or payer review makes them impossible to ignore.
Practices dealing with ChiroTouch Cloud migration errors that require a human biller to resolve are particularly exposed during this window. Migration creates configuration disruption. Configuration disruption creates credential gaps. Credential gaps create silent claim failures. Breaking that chain requires someone who knows where to look — and who knows the difference between a software configuration issue and a documentation problem.
| Regulatory Area | Software-Only Response | Embedded Partner Response |
|---|---|---|
| MFA credential sync | System-level authentication; may not alert on desync | Active monitoring of clearinghouse authentication status |
| SDOH coding requirements | Code set updates applied at system level | Active review of payer contract requirements vs. submitted codes |
| Medicare AT modifier | Format validation on submission | Pre-submission documentation review plus pattern monitoring |
| LCD updates | Fee schedule and rule set updates | Applied to claim language and appeal strategy in real time |
FAQ
Why Does My ChiroTouch Dashboard Show Claims as "Sent" When My Collections Aren't Growing?
"Sent" is a local status update inside your ChiroTouch software. It confirms the claim left your EHR — it does not confirm clearinghouse acceptance, payer receipt, or adjudication outcome.
Claims can show "Sent" while silently failing at the clearinghouse due to credential desyncs, EDI formatting errors, or payer-specific enrollment mismatches. When this happens, the claim doesn't reach the payer, no denial is generated, and the failure becomes visible only when payment doesn't arrive — or when a manual audit of the clearinghouse transmission log identifies the gap.
If your dashboard shows green across the board but AR is growing in the 60–90+ day range without corresponding denials to explain it, clearinghouse-level silent rejections are a likely cause. It's one of the most common revenue leaks in integrated billing environments — and one of the hardest to see without someone actively looking for it.
What Is the "Integrated Trap" in Chiropractic Billing?
The Integrated Trap is the assumption that because your EHR handles claim submission, your billing is being handled.
Submission is the first step in the revenue cycle, not the last. An integrated platform automates throughput — claims go out fast and in volume. What it doesn't automate is the forensic work required after submission: ERA reconciliation, denial investigation, appeal management, underpayment disputes, and the human judgment needed to understand why a denial occurred and whether it's reversible.
When practices treat integrated billing as full revenue cycle management, the gap between those two things fills up quietly in their AR. High-friction denials age past the appeal window. ERAs go unreconciled. Underpayments post as accepted. The collections ceiling never moves.
Does ChiroTouch's Integrated Service Handle Medical Necessity Appeals for Medicare?
Most integrated billing models are designed for submission volume, not appeal depth. Medical necessity appeals for Medicare chiropractic claims require a clinical narrative specific to the patient's record and the payer's current local coverage determination — not a generic redetermination form.
The AT modifier requirement for active care documentation means that Medicare denials on chiropractic claims often can't be resolved with a resubmission alone. The documentation has to tell the clinical story in the language the payer's reviewer needs to approve the claim. That's a skilled task that can't be systematized across a volume-first model.
Is It More Expensive to Use an Embedded Billing Partner Than Integrated Billing?
The software fee for integrated billing may be lower. The question is what that fee includes and what it doesn't.
If your practice is recovering 85 cents of every dollar billed and the gap is sitting in high-friction denials that aren't getting worked, the difference between your current arrangement and a performance-based partner is smaller than the revenue gap. Performance-based billing scales with what's actually recovered — not what's submitted.
The real comparison includes the 90-day AR sitting unworked, the denials that aged past their appeal window, and the underpayments that posted as accepted without anyone checking the contracted rate. That math is worth running before the software fee becomes the deciding factor.
Can Bushido Billing Work Inside My Existing ChiroTouch Cloud Instance?
Yes. Bushido Billing operates as an embedded partner inside your existing ChiroTouch environment. Your clinical workflow doesn't change. Your software configuration stays as-is.
What changes is the billing operation running inside that software — a dedicated biller assigned to your account, active management of your denial queue, weekly billing updates, and human reconciliation of every ERA. The platform is yours. The operation running inside it becomes Bushido's responsibility.
For practices currently working through common data transfer errors in chiropractic EHR migrations or an EHR data migration revenue leakage audit, the embedded model is especially valuable during the transition period when billing disruption risk is highest.
When Should I Audit My Current Billing Operation Rather Than Just Switching Providers?
When you're not sure whether the gap is a provider problem or a process problem.
An audit answers that before you make any operational change. It identifies what's in your AR, which claims are still workable, and what's actually driving the denial pattern. For most practices, that conversation surfaces the answer quickly — if the same denial codes keep appearing across multiple payers and no one's flagged it as a pattern, the problem is structural, not incidental.
A practice assessment through Bushido covers your full billing operation, not just claim volume, and shows you the specific gap between what you're collecting and what's collectible.
What Happens to My AR if I Switch From Integrated Billing to Bushido?
Existing AR doesn't disappear when you switch billing partners. Bushido's AR Cleanup & Recovery service handles the transition — auditing current aging claims, identifying which are still workable within timely filing windows, and initiating appeals or resubmissions on recoverable accounts.
The transition period is where most practices leave the most money behind, because the handoff between billing models creates a gap in active management. Bushido closes that gap as part of the transition — not as a separate engagement.
Conclusion: The Difference Between Submitting Claims and Getting Paid
Integrated billing is a feature of your EHR software. Revenue protection is a different function.
If your current operation submits efficiently and collections reflect it — healthy AR, manageable denial rate, no growing 90-day bucket — integrated billing may be working exactly as intended for your practice. That's a real outcome for documentation-clean practices with straightforward payer profiles.
But if the dashboard says everything is fine and the bank account disagrees, that's not a setting to adjust or a software version to update. It's the absence of a billing operation built to protect your revenue after the claim leaves — not just to confirm it departed.
The billing industry measures performance by submission speed. Revenue protection requires a different measurement entirely.
Bushido Billing is for the practice that's done accepting "we submitted it" as a complete answer. Every claim, every cycle — with a dedicated biller whose job doesn't end when the status turns green.
Knowing your software works is one thing. Knowing your billing works is different.
A practice assessment reviews your full billing operation — not just your claims volume — and shows you exactly what's being recovered and what's being left behind.
Book a Call to see how your current billing actually stacks up.
Software compatibility is the floor. Revenue recovery is the ceiling. The practice that knows the difference is the one that closes the gap.

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet