

Should You Stay on ChiroTouch Server or Move to a New Billing Partner in 2026?
The honest answer is that staying on ChiroTouch Server is a defensible choice — but only if you understand exactly what that choice costs you. Moving to a new billing partner is a smarter move for most practices, not because of the software, but because the billing model underneath the software is what's actually failing.
In 2026, ChiroTouch Server is no longer receiving the protocol-level updates that secure healthcare data environments require. It lacks native MFA enforcement and runs on aging TLS and SQL infrastructure that security researchers have flagged as a primary ransomware entry point for healthcare organizations. That's a compliance and data risk — separate from your billing performance, but compounding it.
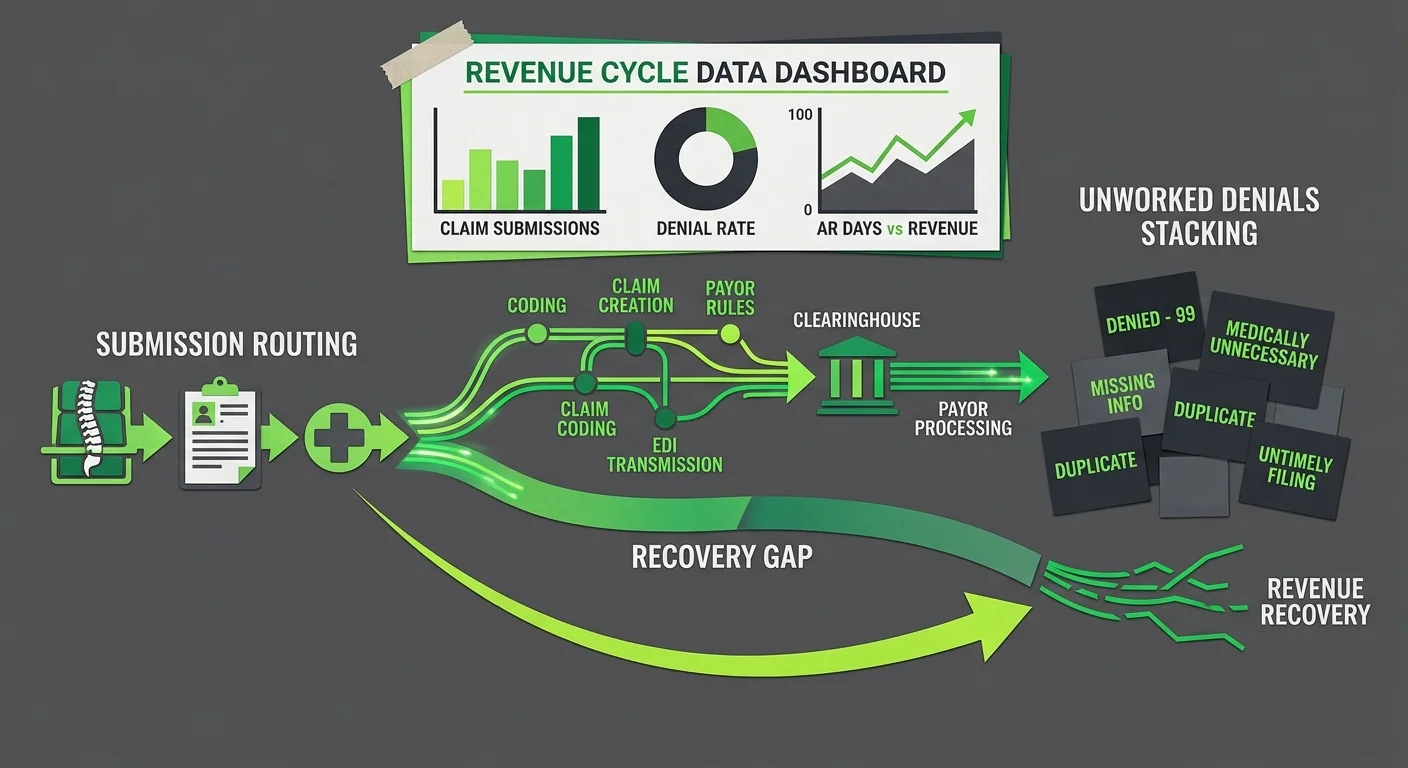
The billing question and the software question are related, but they're not the same question. Your EHR is a submission tool. It routes claims. A specialized billing partner is the team that recovers what the software can't — the denied claims, the unworked AR, the aging balances your current setup treats as acceptable loss.
Most practice owners asking this question are actually trying to solve a revenue problem. They're not EHR engineers. They don't want to become experts in cloud database migrations. They want to know: will this change fix what's broken? This article walks through both paths — staying on Server, migrating to Cloud, and what a specialized billing partner actually does in either scenario — so you can make the decision with full information.
Last Updated: April 20, 2026
- What ChiroTouch Server Is Actually Doing to Your Revenue in 2026
- The Real Risks of Staying on ChiroTouch Server
- What ChiroTouch Cloud Migration Actually Fixes — and What It Doesn’t
- What a Specialized Billing Partner Does That Software Cannot
- How to Know If You’re a Price Shopper or a Revenue Partner Candidate
- Frequently Asked Questions
- Can I stay on ChiroTouch Server indefinitely in 2026?
- Does ChiroTouch Cloud automatically fix my billing denials?
- What is the “Legacy Trap” in chiropractic billing?
- Why do I need a “ChiroTouch Cloud Specialist” specifically?
- Will a new billing partner help me with the migration itself?
- What should I audit before switching billing partners?
- How does the Server vs. Cloud decision affect my revenue cycle management strategy?
- Conclusion
What ChiroTouch Server Is Actually Doing to Your Revenue in 2026
Most practice owners frame this as a technology question. Speed. Local data. Control. Those aren't wrong considerations — but they're the wrong frame for a billing decision.
The right question isn't whether ChiroTouch Server still runs well. It's what's happening to your revenue while you're focused on whether it does. And in 2026, that answer looks different than it did three years ago.
This is why full-service chiropractic billing treats the EHR and the billing operation as two separate conversations. They overlap. But conflating them is how a practice ends up with a smooth-running system and a quietly deteriorating collection rate.
Why “Working Fine” Isn’t the Same as “Working Well”
ChiroTouch Server does what it was designed to do. It captures encounter data. It routes claims. It's fast, it's familiar, and your team knows how to use it.
That's a submission story.
What it's not is a recovery story. And recovery is where chiropractic practices lose revenue.
According to Medicare Improper Payments 2025 data from CMS, the national improper payment rate for fee-for-service Medicare sits at 6.55%. For chiropractic specifically, that rate has historically hit 33.6% — driven by documentation gaps, not submission errors. Faster claim routing doesn't fix documentation. Software doesn't fix documentation. A billing team actively working claims at the clinical level does.
ChiroTouch Server gets the claim out. When it comes back denied — a modifier issue, a medical necessity gap, an AT modifier problem — Server's job is finished. What happens next depends entirely on who's catching it and how fast.
Most practices on Server aren't catching it fast enough.
The Legacy Trap: How Inertia Becomes a Billing Strategy
The legacy trap isn't about software. It's about decisions that stopped being made.
Staying on ChiroTouch Server because nothing is obviously broken is a strategy — it's just not a conscious one. EHR Transition & Data Integrity research published via PubMed (NIH) confirms that EHR transitions carry real financial risk: data mapping errors, payment continuity disruptions, ledger integrity issues. That fear is legitimate.
But the cost of staying accumulates quietly.
Unpatched systems. Coding parameters that haven't kept pace with current payer requirements. Denial patterns that repeat because no one has the bandwidth to trace them to their source. The practice feels stable because claims are going out and cash is coming in. The AR tells a different story.
Submission speed is the metric the software optimizes for. Submission speed is not the metric your revenue depends on.
The Real Risks of Staying on ChiroTouch Server
The risks of staying on a legacy EHR in 2026 aren't hypothetical. They're documented. They show up in two places that most practice owners don't think about until something goes wrong: security exposure and compliance drift.
Both are independent of whether your front desk is using the system well.
Security Abandonment: What Happens When Support Phases Out
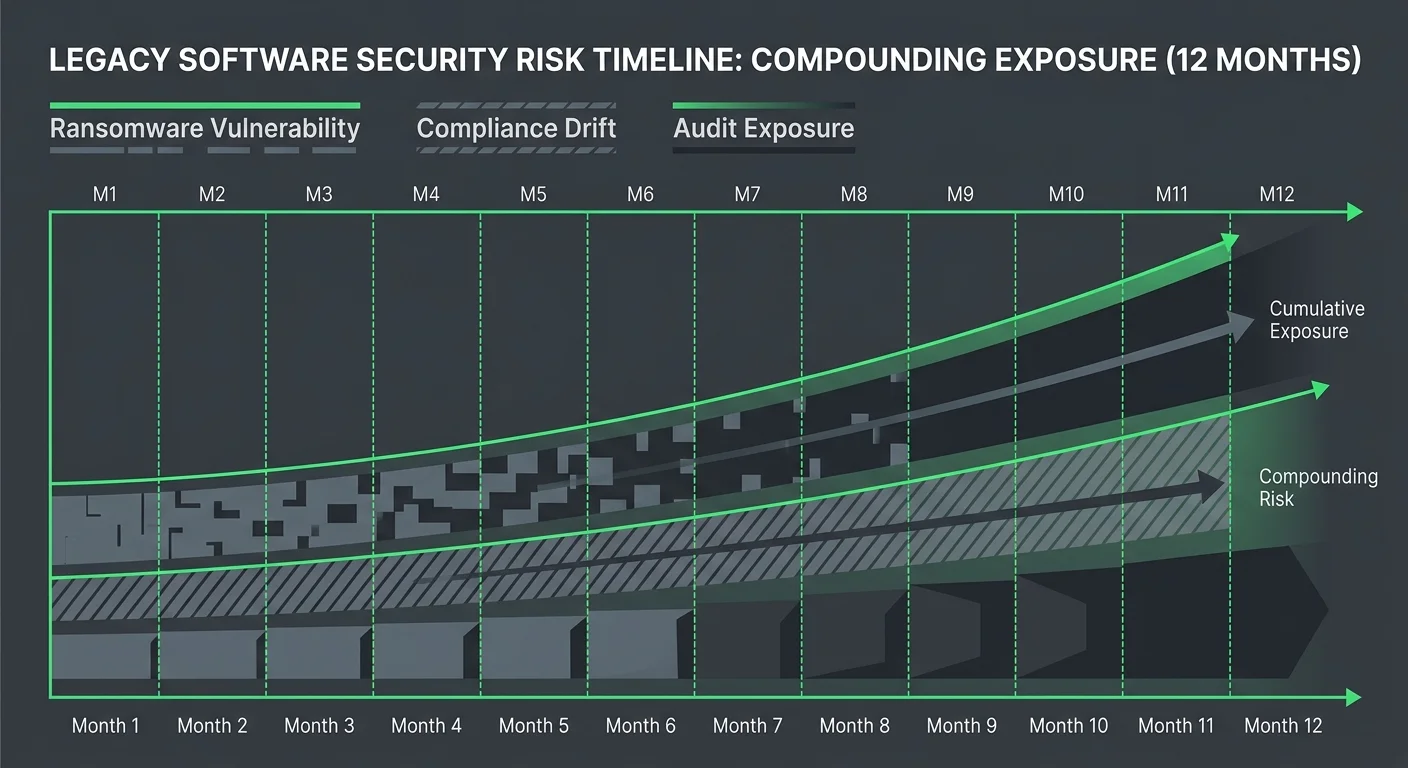
Legacy Software Risks 2026 research from Atiba identifies unpatched SQL databases and outdated TLS protocol versions that function as entry points for automated ransomware targeting healthcare organizations. These aren't edge cases. They're the documented pathways that healthcare practices on legacy infrastructure are being attacked through right now.
ChiroTouch Server doesn't receive the same security update cadence as the Cloud environment. MFA isn't natively enforced at the protocol level. OAuth 2.0 — now standard for compliant API-connected healthcare systems — isn't available on the Server architecture.
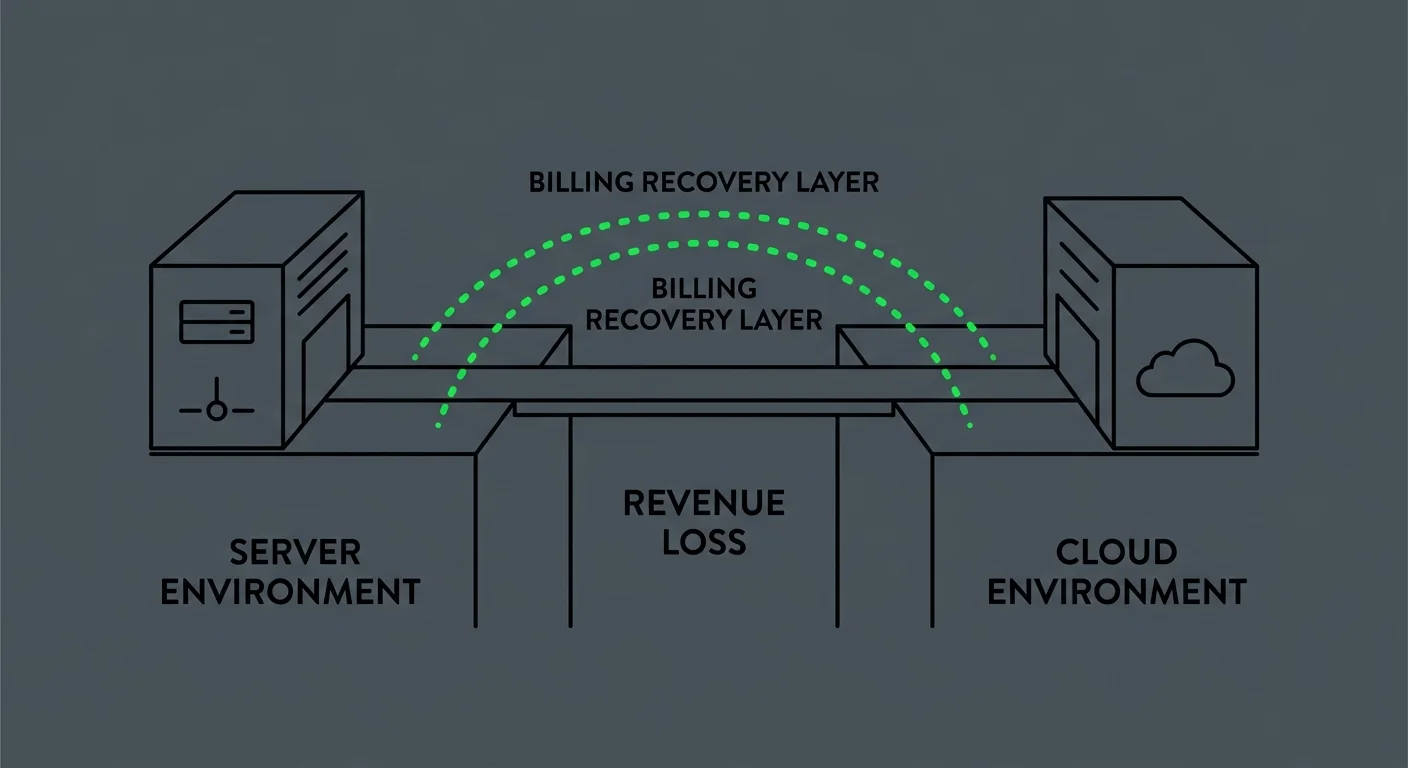
Here's what that means for your billing operation specifically: a ransomware event doesn't lock just your clinical records. It locks your ERA files, your unposted payments, your aging AR reports. Billing recovery from a ransomware event runs in weeks, not days. And the revenue lost during that window is rarely fully recovered.
- Security drift (unpatched vulnerabilities) — Legacy environments missing regular patch cycles are flagged as high-risk healthcare infrastructure, a classification that increasingly touches insurance credentialing and payer relationships in 2026.
- Data integrity exposure (unencrypted local storage) — Server environments storing PHI locally without current encryption standards are non-compliant with evolving HIPAA data-at-rest guidance.
- Ransomware targeting (automated attack vectors) — Healthcare practices on legacy platforms carry higher attack ROI for bad actors — they're more likely to pay, and recovery takes longer.
Understanding how ChiroTouch Cloud Specialists manage the security transition is worth reviewing before you decide to hold course on Server.
Compliance Drift and Chiropractic Audit Exposure
Security exposure is the visible risk. Compliance drift is the slow-burn one.
Chiropractic billing operates in a high-scrutiny Medicare environment. AT modifier use, subluxation documentation, active vs. maintenance care distinctions — these requirements don't stay still. They shift with coverage determination updates and payer policy changes. Software that isn't receiving protocol-level updates enforces the parameters it was built with, not the ones that apply now.
Medicare Improper Payments 2025 data from CMS shows a 6.55% national FFS improper payment rate, with chiropractic at a historically disproportionate rate due to documentation failures — not submission failures. A practice running on aging infrastructure, without a billing team actively reviewing claim-level documentation against current standards, carries exactly the audit exposure that statistic reflects.
The software version isn't the problem. The billing problem is the absence of a recovery system working alongside whatever software you're using. That's what full-service chiropractic billing addresses — not the platform, but the recovery operation on top of it.
| Risk Category | ChiroTouch Server 2026 | ChiroTouch Cloud 2026 |
|---|---|---|
| Security update cadence | Reduced or discontinued | Active via vendor |
| MFA enforcement | Not natively enforced | Available |
| TLS/SQL patch status | Legacy versions | Current versions |
| Ransomware exposure | Elevated | Reduced |
| Coding compliance enforcement | Software-dependent only | Software-dependent only |
| Active claim recovery | Requires separate billing team | Requires separate billing team |
What ChiroTouch Cloud Migration Actually Fixes — and What It Doesn’t
The migration pitch you're hearing from vendors is a security pitch. More secure. More compliant. Better infrastructure. All of that is true.
What it isn't is a billing pitch. And that gap matters.
The Submission Environment vs. The Recovery Operation
Here's the distinction that doesn't show up in any migration brochure: Cloud changes where your claims are submitted from. It doesn't change what happens after they come back denied.
When you move from Server to Cloud, you change the submission environment. The credential configuration, the API routing, the data storage layer — all of that upgrades. But if your billing team wasn't working denials effectively before the migration, they won't start after it. The Cloud doesn't fix the recovery operation. Only the people running the recovery operation can do that.
RCM Trends 2026 analysis from RCM Workshop confirms that strategic billing partnerships are increasingly replacing ad-hoc software vendor relationships as interoperability and regulatory pressure grow. The practices performing best on revenue aren't the ones who upgraded their EHR first. They're the ones with a dedicated team working what the software can't touch.
ChiroTouch Cloud gives you a stronger platform. For a direct comparison of what each environment delivers at the billing level, see the ChiroTouch Server vs. Cloud billing comparison.
- Submission accuracy (software's job) — Both Server and Cloud submit claims. Clean claims process through either platform. The submission environment isn't where most chiropractic revenue disappears.
- Denial recovery (billing team's job) — Complex denials, underpaid claims, medical necessity disputes, and aging balances require human judgment. Neither Server nor Cloud performs this function.
- ERA reconciliation (billing team's job) — Unposted payments, unlinked ERAs, and split-payment scenarios are manual recovery tasks. Software routes the transaction. A billing team closes the loop.
Why Cloud Migration Without a Billing Partner Often Creates New Problems
The migration window is where practices are losing revenue right now — not because Cloud is bad, but because the transition itself creates a vulnerability that nobody's billing setup is built to manage alone.
EHR Transition & Data Integrity research from PubMed (NIH) documents that data mapping errors during platform transitions create significant financial continuity risk. Patient ledgers migrate imperfectly. ERA files from the Server environment don't automatically port. Claims submitted in the final days before cutover get adjudicated during the Cloud setup period and fall through the gap — submitted under Server, resolved during transition, never reconciled on either side.
These are the "silent rejections." Claims that technically went out but never came back in any way that triggered follow-up.
A migration without a billing software compatibility review and a pre-migration AR audit leaves that revenue behind permanently. Most billing vendors don't build this into their onboarding. Most in-house billing teams don't have bandwidth for it during an active transition.
| Migration Phase | What Goes Wrong | What a Billing Partner Does |
|---|---|---|
| Pre-migration | Unworked AR left on Server | Full AR audit before cutover |
| Cutover window | ERA files unlinked from new system | Reconciliation monitoring during transition |
| Post-migration | Legacy claims fall through | Active follow-up on all pre-migration claims |
| Ongoing | New system, same billing gaps | Denial recovery and weekly AR review |
What a Specialized Billing Partner Does That Software Cannot

The difference between a ChiroTouch Cloud Specialist and a general billing service isn't a marketing distinction. It's an operational one.
A generalist knows how to route claims through the platform. A specialist knows where the platform breaks — specifically, predictably, and in the patterns that cost practices the most revenue.
The Forensic Architect Role During Migration
"Forensic architect" describes something specific: auditing the full billing history before, during, and after a platform transition so nothing gets permanently abandoned in the handoff.
Three things consistently go wrong in migrations without active billing oversight:
- Unlinked ERAs — Remittance files from the Server environment don't port automatically. Without manual reconciliation during the transition window, the payments they represent are never posted to the new system.
- Pre-migration denial follow-up — Claims submitted in the final days on Server get adjudicated while the team is focused on Cloud setup. Denials come back to an inbox that's not watching for them, and they age past the filing deadline before anyone notices.
- Patient ledger mapping errors — Data that migrates imperfectly creates billing discrepancies that don't surface until weeks after cutover — long after the transition itself has been declared complete.
A billing partner managing this process works between what the old system saw and what the new system needs to see. That's not a software capability. That's clinical and operational expertise applied at the transition layer.
Active Revenue Defense vs. Passive Claims Submission
Most billing operations — in-house or outsourced — run as submission operations. Claims go out. Payments come in. What falls through the middle is tracked loosely, or not at all.
Active revenue defense treats every denial, every underpayment, and every aging balance as a workable problem — not an acceptable loss.
The practices recovering the most revenue aren't the ones submitting the most claims. They're the ones with someone on the other side of the denial, working it back. The 15% that gets denied. The underpayments that look like approvals until someone compares them against the fee schedule. The "pending" claim at day 45 that should have been followed up at day 30.
Software submits. It doesn't call the payer. It doesn't flag the underpayment. It doesn't identify the documentation pattern behind a recurring denial and trace it back to the clinician's notes so it stops happening.
That's billing. And it's what a partner does.
How to Know If You’re a Price Shopper or a Revenue Partner Candidate
Not every practice is the right fit for this model. Saying so clearly is more useful than pretending otherwise.
There's a specific type of practice owner this partnership is built for. And there's a type it isn't. Knowing which category you're in before the conversation starts saves time on both ends.
Who This Partnership Is Built For
The right fit is the practice owner who's stopped assuming their current billing is recovering everything it should — and wants to find out specifically what isn't.
That person isn't leading with "what's your rate?" They're asking: "What does your denial follow-up process look like? How do you handle ERA reconciliation? What happens to my AR during the transition?" Those are revenue questions. They're the questions that actually predict billing performance.
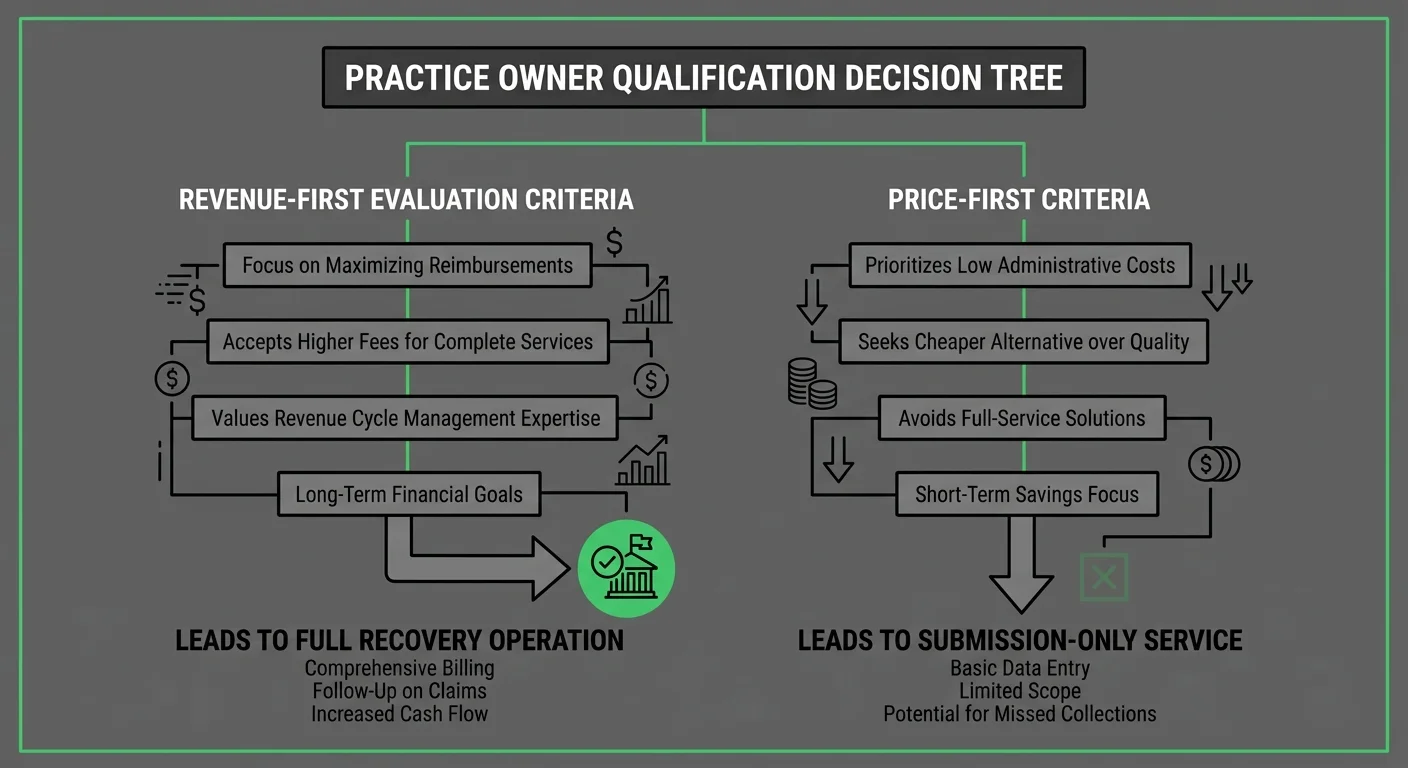
- Revenue-first practices — Owners who track collection rate and denial recovery, not just claims volume and submission turnaround. These practices already know something is being left behind. They want to find it.
- Practices mid-migration or post-migration — Clinics that recently moved to Cloud and sense something changed in their cash flow but can't pinpoint where. The transition window is almost always where it happened.
- Practices with aging AR — Clinics carrying 90+ day balances that aren't being worked systematically. The software version doesn't matter here. The recovery operation does.
- Practices with recurring denials — The same denial codes, same payers, same reason — month after month. That's a documentation or coding pattern, not a submission error. Software won't fix it.
Who This Isn’t For
If the first question is about rate, this isn't the right fit — and that's okay to say out loud.
Rate matters. It's not the wrong thing to ask. But if rate is the primary evaluation criterion, the conversation never reaches the question that actually determines revenue performance: what percentage of denied and underpaid claims are being recovered, and in what timeframe?
A practice optimizing for the lowest billing percentage will get that number and accept the revenue lost to unworked denials as the cost of a cheaper service. That's a valid trade. It's not the trade that maximizes collections.
- Price-first decision makers — If the goal is minimizing billing cost rather than maximizing recoverable revenue, a performance-based model won't align. The math only works in the partner's favor when claims are being fully recovered, which requires active work — not passive routing.
- Practices that don't want visibility into their billing — A partner working your AR will surface what's been missed. Some practice owners aren't ready for that information. That's not a criticism. It's a fit issue.
- Practices expecting a hands-off service — Active recovery requires collaboration: documentation feedback, weekly AR reviews, communication about what's recurring. If the expectation is set-it-and-forget-it, this partnership won't deliver what either side needs.
Frequently Asked Questions
Can I stay on ChiroTouch Server indefinitely in 2026?
Technically, yes. No regulation forces a migration on a specific timeline.
But the question worth asking isn't "can I stay?" It's "what does staying actually cost?"
Legacy Software Risks 2026 research from Atiba identifies unpatched SQL and outdated TLS versions as the primary automated ransomware entry points in healthcare IT environments. That risk doesn't stay static — it compounds each month without a patch cycle.
The billing impact is specific: a ransomware event on a Server environment locks your ERA files and your unposted payments alongside your clinical records. Billing recovery takes weeks. Revenue lost during that window rarely comes back. If you're staying on Server, you need a security and billing monitoring plan that accounts for this — and most practices don't have one.
Does ChiroTouch Cloud automatically fix my billing denials?
No. This is the most expensive misconception driving migration decisions in 2026.
Cloud upgrades the submission environment. It doesn't upgrade the recovery operation. Denial management, ERA reconciliation, underpayment follow-up — these are human billing functions. Neither Server nor Cloud performs them.
Practices that migrate to Cloud expecting their denial rate to improve are routinely disappointed. The same patterns that existed on Server reappear in the new environment within 60–90 days, because the pattern was never about the platform. It was about the recovery operation — or the absence of one.
If you're migrating to Cloud, evaluate your billing operation at the same time. The migration is the opportunity to fix both, and that window doesn't stay open.
What is the “Legacy Trap” in chiropractic billing?
It's the cycle of staying on aging software to avoid migration pain, while slowly losing revenue to the compounding effects of outdated coding standards, unworked AR, and security exposure that nobody's explicitly monitoring.
It feels like stability — because claims are going out and cash is coming in.
But the relevant comparison isn't where you are versus where you were. It's where you are versus where a fully-functioning billing operation would put you. Practices that discover the legacy trap usually do so when they switch billing partners and the incoming team flags months of unworked denials and aging balances that were being treated as write-offs.
For more on what platform-specific expertise looks like in practice, review ChiroTouch Cloud Specialists.
Why do I need a “ChiroTouch Cloud Specialist” specifically?
A generalist billing vendor can submit claims through ChiroTouch Cloud. A specialist understands where that platform specifically fails — the ERA reconciliation patterns that break during migration, the credential configurations that affect claim routing, the MFA and API setup issues that create silent rejections nobody catches.
The practical difference shows up during and after a migration. A generalist starts their work after the platform is set up. A ChiroTouch Cloud Specialist audits the transition itself — tracking pre-migration claims through adjudication, reconciling ERAs that didn't port cleanly, and catching the revenue that falls through the transition gap.
That gap is real. And it's where the specialist earns the distinction.
Will a new billing partner help me with the migration itself?
A specialized billing partner with direct ChiroTouch environment experience works the transition as a forensic process — auditing the data transfer, tracking unlinked ERAs, following up on pre-migration claims, and making sure no patient ledger gets permanently abandoned between Server and Cloud.
Generic billing services typically begin their engagement after the migration is complete. By then, the transition-window revenue is already gone.
If you're evaluating billing partners during a migration, the right question is: "What does your pre-migration audit look like, and what's your protocol for transition-window claim follow-up?" If the answer doesn't include pre-migration AR review, the onboarding starts after the most vulnerable period has already passed. Review how human billers fix ChiroTouch Cloud migration errors to understand what that oversight specifically involves.
What should I audit before switching billing partners?
Before any transition — regardless of platform — have clear answers to these four questions:
- What's your current denial rate by payer and by denial reason code?
- How much AR is sitting past 90 days, and which claims in that bucket are still workable?
- Are all ERAs from the past 90 days posted and reconciled?
- Are there claims from the past 60 days with no adjudication response?
These four answers reveal the actual state of your current billing operation. A billing partner worth working with will ask these questions before onboarding — not after. If your current billing team can't answer them, that's useful information in its own right.
How does the Server vs. Cloud decision affect my revenue cycle management strategy?
The platform decision creates two specific risks: security exposure on Server, and migration-window revenue vulnerability during a Cloud transition.
RCM Trends 2026 from RCM Workshop confirms that RCM strategy is shifting toward billing partnerships that provide both platform expertise and active recovery operations — not just claim submission through whichever EHR the practice is running.
The practices navigating this well are treating the software decision and the billing decision as separate evaluations with separate criteria. Platform choice determines your infrastructure risk. Billing partner choice determines your revenue performance. Conflating them is how practices migrate to Cloud and still end up with the same AR problem six months later. For a direct comparison of what each platform delivers at the billing level, see the ChiroTouch Server vs. Cloud billing comparison.
Conclusion
This was never really a software question.
The practices that recover the most revenue aren't the ones who made the right platform choice. They're the ones who stopped treating their billing software as their billing strategy.
Submission is not billing. Getting paid is billing. ChiroTouch Server submits your claims. ChiroTouch Cloud submits your claims. Neither one follows up when a claim comes back denied, catches the underpayment that looks like approval until you compare it to your fee schedule, or traces the recurring AT modifier problem back to a documentation pattern that needs to change at the point of care.
That's what a billing partner does.
In 2026, the decision to stay on Server or migrate to Cloud matters — for your security posture, for your compliance exposure, for your infrastructure risk. But the decision that determines your revenue performance is the one about your billing operation. That decision is separate. It's more important. And it doesn't automatically get made when you upgrade your platform.
If you've been treating your EHR upgrade as your revenue strategy, this is the moment to separate those two conversations. The platform question has a right answer that depends on your infrastructure tolerance. The billing question has a right answer that depends on whether the people working your claims are actually working them — or just routing them.
Your software routes claims. Your billing partner recovers them.
A practice assessment shows you exactly what's being recovered right now — and what's sitting in aging AR that still has a workable window.
See how your billing actually stacks up before your next platform decision locks you into the same recovery gap with a different interface.
Every week of unworked AR is a week that balance ages past the point where it can be recovered. The platform you run it through doesn't change that math.

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet