

ChiroTouch Server vs. Cloud: Which Platform is Better for High-Volume Billing in 2026?
For high-volume chiropractic practices in 2026, neither ChiroTouch Server nor ChiroTouch Cloud is the better "billing platform" — because neither one is a billing platform. Both are claim submission tools. Server offers faster local processing, deeper ledger customization, and better handling of complex personal injury (PI) cases. Cloud offers remote access, automatic regulatory updates, and vendor-supported infrastructure going forward. That comparison is where most reviews stop. The part that actually determines whether a high-volume practice gets paid sits underneath it. The platform decision affects data entry speed, remote access, regulatory update cadence, and how historical ledger data carries forward. It does not determine denial rate, AR recovery, or how much of the complex revenue actually gets collected. Those outcomes come from whoever is reading the denials, writing the appeals, and following up on the claims — not from where the EHR is hosted. High-volume practices carrying PI lien cases or Medicare patients with active-care documentation requirements are the ones most exposed during a Server-to-Cloud migration. Ledger structures change in the new environment, historical claim data can distort during transfer, and unworked AR becomes easier to lose track of during the transition than it is in steady-state operations. This article covers the full comparison: where Server still wins, where Cloud closes the gap, what high-volume practices lose in the migration, and how to audit for revenue leakage during the switch — including what the platform decision does and does not change about actual billing outcomes.
Last Updated: April 20, 2026
The Real Question Behind Server vs. Cloud
Most practice owners come into this comparison looking for a software answer. They're holding a billing question.
The decision isn't really Server vs. Cloud. It's whether full-service chiropractic billing — whoever's running it, wherever the EHR lives — is actually recovering the revenue the practice is producing. The migration pressure from the vendor just forces the question into the open.
That's a different conversation than "which version should I buy." It's also the only one worth having.
Why the Comparison Usually Gets Framed Wrong
Most Server-vs-Cloud breakdowns measure the wrong things. Processing speed. Interface feel. Upgrade cadence. Mobile access.
Those are real differences. None of them determines what gets paid.
Billing companies measure the same way. Submission speed. Claim volume. How fast claims go out the door. Those numbers describe activity — not outcomes. The gap between "submitted" and "collected" is where high-volume practices lose the most revenue, and the EHR platform has almost nothing to do with it.
The claims that actually need someone's attention aren't the clean ones. Medical necessity appeals. Multi-step denials. PI lien documentation. AT modifier corrections.
Those are the claims that get abandoned in volume-first billing — they cost more to work than a throughput model allows. The Cloud doesn't fix that. Neither does the Server. The platform sends the claim. Someone still has to fight for the payment when the payer says no. That's active revenue defense — and it's a human function, not a hosting model.
What the Platform Decision Actually Affects
Four things. That's the list.
What actually changes:
- Data entry speed (front desk throughput) — Server runs on your LAN and feels instantaneous. Cloud performance depends on bandwidth and vendor server load, which varies.
- Remote access (staff across locations) — Cloud is native and browser-based. Server requires VPN, remote desktop, or whatever workaround IT set up years ago.
- Regulatory update cadence (ICD-10, CPT, payer rules) — Cloud receives vendor updates automatically. Server depends on manual install schedules that tend to slip.
- Historical ledger carry-forward (existing claim data) — Server's legacy structure stays put. Cloud's structure is where transfer risk lives during the migration itself.
That's what changes.
Denial rate doesn't change because of the platform. AR aging doesn't change because of the platform. Whether anyone is working the unpaid claims doesn't change because of the platform. Those outcomes depend on who's reading the denial reason, who's pulling the documentation, who's writing the appeal — regardless of which ChiroTouch environment the claim came from.
Practices that make the platform decision in isolation tend to discover this later. Usually 90 days in, when the AR report looks worse than expected and nobody can quite explain why. At that point, choosing chiropractic billing software becomes the wrong focus — the billing operation is the one that needs the audit.
ChiroTouch Server vs. Cloud: Head-to-Head Comparison
This is where the actual differences live. Server and Cloud vary in how they handle high-volume environments, and those differences matter.
What they don't vary on is what they require from the billing team. That part stays the same, regardless of where the software lives.
Processing Speed and Local Performance
Server runs on your local network. Data entry, ledger lookups, claim queuing — all of it happens at LAN speed. In a busy clinic, that's the difference between a front desk that moves between patients and one that stalls.
Cloud runs over the internet. Performance depends on your bandwidth, the vendor's server load, and whatever browser your staff is using that week. ChiroTouch Reviews 2026 data on Capterra documents what practices describe as "clicky" interfaces, page reloads between actions, and lag that wasn't there before.
At 40 patients a day, it's an irritation.
At 120 patients a day with multiple providers entering simultaneously, it compounds. Throughput slows. Office managers burn out. Those costs don't show up in a vendor dashboard — but they're real, and ChiroTouch Cloud specialists who've worked the environment at volume see them immediately.
Remote Access, Updates, and Vendor Support
Cloud wins three areas cleanly:
- Native remote access (no workaround required) — Staff log in the same way from home, between locations, anywhere — without VPN, remote desktop tools, or an IT call when something breaks.
- Automatic regulatory updates (vendor pushes them) — ICD-10 additions, CPT changes, and payer rule adjustments arrive without pulling IT into a local install schedule.
- Primary vendor development focus (ongoing investment) — The product roadmap is concentrated here, which means legacy Server parity is no longer the priority going forward.
Server's trade-off is the other side of the same ledger. Local control, local performance — but you own the updates, the backups, and the infrastructure.
For 2026 and beyond, Server owners should expect declining vendor investment in the legacy environment. That's the forcing function behind most migrations — not a software improvement. Whether the migration comes with ChiroTouch Cloud specialists who understand the billing side of the transition, or just an IT vendor spinning up the new environment, shapes what the first 90 days after the switch actually look like.
| Capability | ChiroTouch Server | ChiroTouch Cloud |
|---|---|---|
| Data entry speed | Fast (local network) | Variable (depends on bandwidth) |
| Remote access | Limited, requires workaround | Native, browser-based |
| Regulatory updates | Manual or IT-dependent | Automatic push from vendor |
| Ledger customization depth | High — legacy flexibility | Reduced — standardized structures |
| Vendor support trajectory | Declining | Primary development focus |
| PI case ledger handling | Complex cases well-supported | Separation workflows more limited |
| Infrastructure responsibility | Practice owns it | Vendor owns it |
Why "Upgrade the EHR, Fix the Billing" Fails
Here's the assumption that quietly costs practices money.
The migration gets pitched — sometimes by the vendor, sometimes by the practice's own internal logic — as a billing improvement. It's not. Moving to the Cloud doesn't change what the EHR is. It changes where it lives.
EHR software builds the claim. Attaches the codes. Sends the claim out through a clearinghouse. That's submission.
Billing is what happens when the claim comes back. The denial review. The medical necessity argument. The documentation correction. The appeal letter. The follow-up call with the payer next Thursday when nothing's moved.
No EHR does any of that. Not Server. Not Cloud. Not any platform marketing itself as an "all-in-one billing solution." The software generates the claim — someone has to work it when it doesn't pay.
Practices that treat the migration as a billing fix find out about 60 days in. The claims go out through a nicer interface. The denials come back at the same rate. The AR still isn't getting worked. A Revenue Impact Analysis of cloud-based EHR adoption confirms what's already visible in the field — cloud infrastructure alone doesn't reduce denials. Real-time validation and human judgment decide that, not the hosting environment.
The platform changed. The problem didn't. Which means the conversation isn't really about Server or Cloud — it's about whether active revenue defense is happening at all, under either environment.
What High-Volume and PI Practices Actually Lose in the Cloud
High-volume practices have workflows that Cloud handles differently than Server did. No single one is a deal-breaker.
Stacked together, they become the "Cloud feels awkward" experience showing up across 2026 reviews. Each friction point is an opportunity for a claim to get dropped or a ledger to get misread.
Ledger Complexity and PI Case Separation
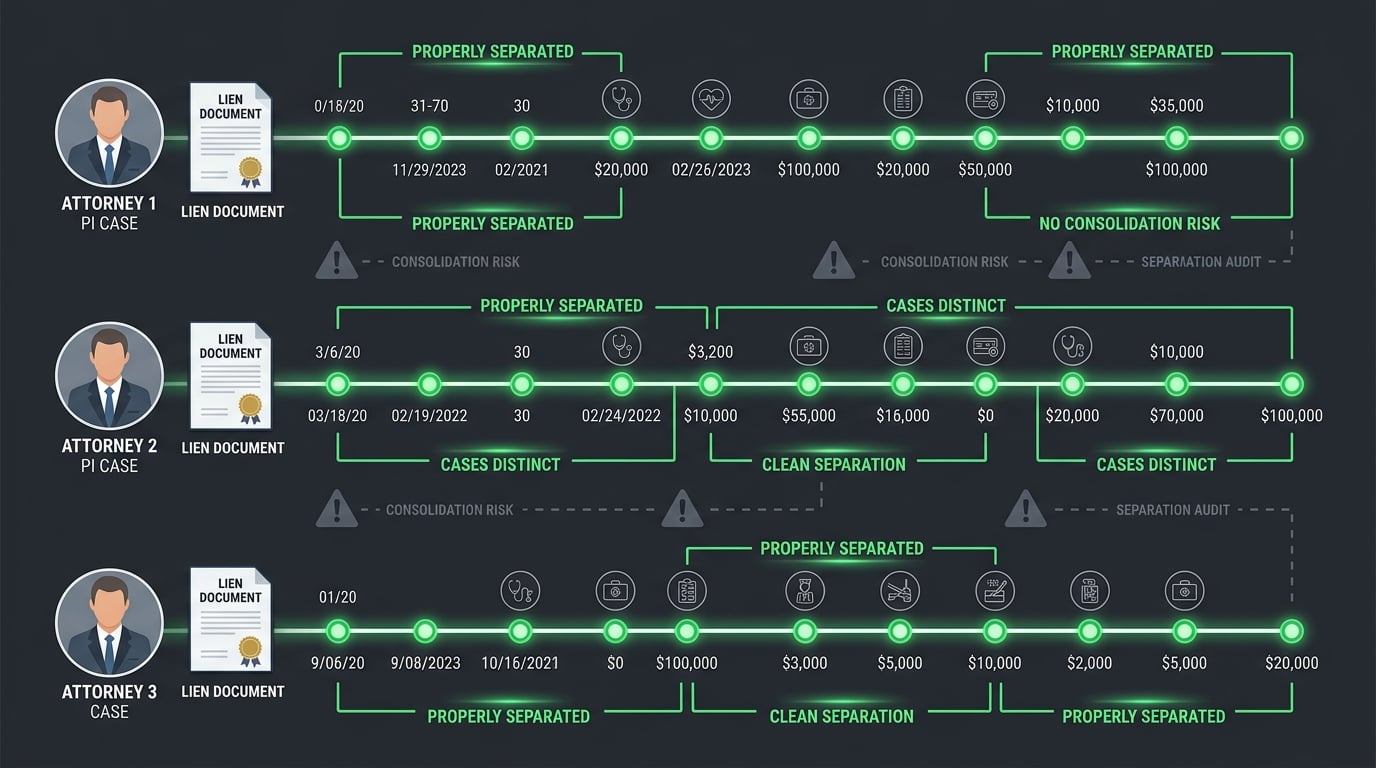
Personal injury billing produces the most complex ledgers in the practice. Full stop.
One patient can carry multiple open cases at once — a current auto accident, a pending workers' comp claim, residual regular insurance activity. Each case has its own attorney. Its own lien. Its own documentation standards. Its own timing.
Server's legacy ledger structure let high-volume PI practices separate those cases manually — and most of them built workflows around it over years. EHR Comparison 2026 review data on Software Advice surfaces the complaint that's been quietly repeating: high-volume practices report difficulty separating PI cases within the Cloud ledger system.
The Cloud standardizes the structure more aggressively. Helpful for baseline reporting. Harder on practices whose PI workflows depended on the granularity.
The risk isn't that PI billing becomes impossible. It's that each of these now requires extra manual steps:
- Attorney lien reporting (case-level documentation pulls) — Workflows that ran cleanly in Server need additional steps in Cloud to produce the same case-specific output.
- Multi-case reconciliation (multiple open cases per patient) — Cloud's standardized ledger structure can consolidate what Server kept separate, so multi-case patients need closer review.
- Documentation pulls under payer pressure (medical necessity arguments) — The access pattern to the underlying note is different, which typically slows appeal work during the first few months.
A rushed office manager skips or simplifies those steps. That's where the missed postings and quiet reconciliation errors start.
This is the single biggest reason PI-heavy practices benefit from ChiroTouch Cloud specialists on the billing side — people who've seen the ledger issues before and know which cases need case-level verification first.
Maintenance vs. Active Care Documentation in a Cloud Workflow
Medicare doesn't cover maintenance care. It covers active treatment. The AT modifier is how the claim tells the payer which one this visit is — and the documentation behind it is what defends the claim when the payer pushes back.
It's one of the most audited areas in chiropractic billing. The CMS Medicare Compliance Tips program documented a 33.6% improper payment rate for chiropractic services, driven largely by documentation issues.
Server or Cloud, the EHR doesn't make the active-vs-maintenance call. The provider's documentation does. What changes between environments is how fast the billing team can pull that documentation when a payer questions medical necessity.
In Server, experienced staff often had direct, fast access to the file. In Cloud, the access pattern is different — sometimes faster, sometimes slower, almost always rearranged.
Teams that learned Server and now work in Cloud go through a productivity dip. Usually three to six months. During that window, denial follow-up slows. Appeals get deprioritized. Revenue that was getting recovered pre-migration stops getting recovered during it.
The practice owner doesn't see it in real time. It shows up in the aging report 90 to 120 days later — by which point the claims requiring active revenue defense have already aged past recovery.
Who This Comparison Isn't For
If your decision between Server and Cloud comes down to which one is cheaper, this isn't the comparison you need.
There are real cost differences. Cloud is typically subscription. Server involves local infrastructure and declining vendor support. Those numbers can be calculated.
But if price is the first and only variable, the conversation is already incomplete.
Neither platform determines how much of your billable revenue actually gets collected. That comes from the billing operation — not the pricing model. Practices shopping for the cheapest billing software and the cheapest billing rate end up with volume-first, automation-forward billing. The kind that walks past exactly the high-complexity claims where a PI-heavy or Medicare-heavy practice keeps its revenue.
That's the wrong fight to be in if you're running high volume.
If rate is the decision, the deciding conversation isn't really about ChiroTouch or about choosing chiropractic billing software. It's about whether the practice is built to defend its revenue or absorb the loss.
Revenue Leakage During Server-to-Cloud Migration
The migration itself is where the money leaves. Not the destination.
Data carries forward. Claim histories carry forward. Patient ledgers carry forward. But "carries forward" and "carries forward accurately" are different things — and the gap between them is usually measured in revenue that quietly disappears during the transfer window.
Data Integrity Risks and Lost Historical Claims
Any environment-to-environment migration introduces data integrity risk. Fields map differently. Legacy customizations don't always translate. Historical claim statuses — especially the "in appeal," "pending resubmission," and "awaiting payer response" ones — can lose their context in the transfer.
The EHR Transition Study published through PubMed Central identifies data integrity issues and "lost data" as significant risks during EHR transitions.
For a practice sitting on 6 to 18 months of unworked AR at the time of migration, this is the moment that AR is most exposed. A claim flagged "awaiting documentation for appeal" in Server can migrate to Cloud as a generic "unpaid" status — then sit in a new aging bucket with no flag telling anyone it needs action.
The claim isn't technically lost. The context is. And the context is what told the billing team to work it.
When that context walks out the door, the practice needs someone who knows what to rebuild. That's usually a conversation about ChiroTouch Cloud specialists versus sticking with a billing operation that doesn't know what it's looking for in the new environment.
The "Unworked AR" Problem in a Migration Window
Neglected AR doesn't recover on its own. It compounds. Ages past the point of return. And the whole time, the practice assumes the biller is working it.
That's true in steady state. In a migration, it's worse.
The transition is a natural break in workflow continuity. Staff are learning the new environment. Reports run differently. Legacy views don't exist anymore. The billing operation's attention shifts from "working the claims" to "learning the system."
During that shift — typically 60 to 180 days — AR that was already neglected gets harder to recover. AR that was being worked slows down because the workflow friction just increased.
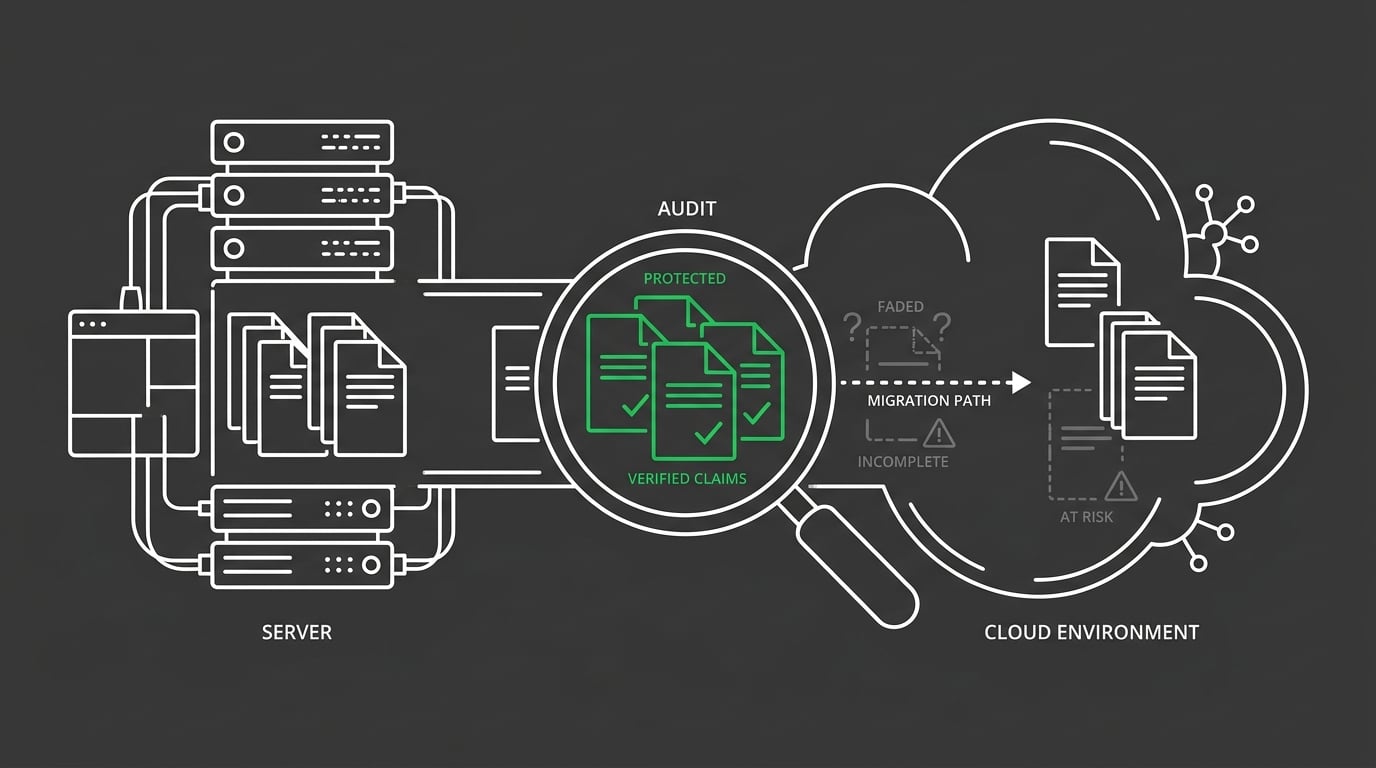
A practice audit before and after the migration is how this gets measured. Before: inventory the current AR, flag it, snapshot every status. After: verify the same claims in the new environment. Anything that didn't transfer correctly surfaces immediately — not six months later when it's too aged to collect.
That audit is also where active revenue defense either stays in place during the transition or quietly stops, depending on who's running it.
What to Audit Before and After the Switch
A practice audit during a ChiroTouch migration is scoped differently than a routine audit. It's looking for transition damage. Not steady-state leakage.
The pre-migration inventory establishes the baseline:
- Total AR by aging bucket (comparison baseline) — Snapshot every bucket before the migration so there's something to reconcile against afterward.
- Open appeals and pending denials (each tagged with current status) — Every claim's workflow state captured so "appeal pending" doesn't flatten into generic "unpaid" in the new environment.
- Active PI case balances (case-level, not patient-level) — Every case separately for every patient carrying multiple, because Cloud's ledger may consolidate what Server kept distinct.
- Medicare claims awaiting documentation (AT modifier notes) — Every claim tied to active-care documentation flagged so the supporting file stays linked through the transfer.
Anything with an active status needs to be accounted for in the new environment within 30 days.
The post-migration audit verifies it transferred. Every claim with an active status should still have an active status. Every appeal in progress should still be in progress. Every aging bucket should reconcile.
Anything that doesn't — that's either a technical transfer issue or a workflow gap. Both get addressed while they're still fresh.
Practices that treat the migration as an IT project skip this audit. That's where the revenue leakage hides. Which is also why some practices end up talking to ChiroTouch Cloud specialists about what their current billing operation actually did during the migration — and what it didn't.
| Migration Risk Area | What Happens | How It's Caught |
|---|---|---|
| Status loss on in-appeal claims | "Appeal pending" becomes generic "unpaid" in new environment | Pre-migration AR snapshot, post-migration reconciliation |
| PI ledger separation breakdown | Multi-case patient ledgers consolidate incorrectly | Case-level review of active PI files before transfer |
| Medicare AT modifier documentation disconnect | Documentation link breaks between claim and supporting note | Post-migration audit of recent Medicare claims |
| Denial queue reset | Active denial work queue doesn't carry forward | Export of denial queue before migration, manual rebuild after |
| Aging bucket reclassification | Claims shift aging buckets due to date field mapping | Full AR aging comparison, pre vs. post |
FAQ: ChiroTouch Server vs. Cloud for High-Volume Billing
Why is ChiroTouch Cloud reportedly slower for high-volume billing than the Server version?
Cloud performance depends on internet bandwidth and the vendor's server load. Server ran on your local network, which traditionally handles high-volume data entry with less latency between actions.
In a 40-patients-per-day practice, you barely notice. In a 120-patients-per-day clinic with multiple providers entering at the same time, the lag compounds — staff frustration, slower throughput, the whole cascade.
The fix isn't only the platform. Bandwidth matters. Browser environment matters. Workflow design matters.
Some of the reported "slowness" is genuine latency. Some of it is a workflow built for Server that hasn't been rethought for Cloud. Teams that don't know the difference usually blame the software. Teams that do — including the billing operations who've become ChiroTouch Cloud specialists by working through the transition with multiple practices — separate the two and address them independently.
Can I keep my ChiroTouch Server version indefinitely in 2026?
Technically, yes — the software keeps functioning. Practically, the vendor's investment is in the Cloud product, and that shift has consequences over time.
Declining support means ICD-10 updates, CPT changes, and payer rule adjustments arrive slower or require manual workarounds. Give it 24 to 36 months and that gap becomes a billing risk — claims coded to outdated standards start getting denied, and the denials are entirely avoidable.
Staying on Server is a defensible short-term decision when the migration timing doesn't work for the practice. It's not a defensible long-term plan.
When the conversation shifts to the long term, it usually merges into a bigger one — choosing chiropractic billing software and evaluating whether the current billing operation can actually work the new environment well.
What are the specific risks of migrating high-volume PI cases to ChiroTouch Cloud?
Personal injury billing relies on case-level ledger separation — each accident, each attorney, each lien tracked independently within a single patient record. Server's ledger structure supported this natively; the Cloud standardizes ledger structures in ways that can consolidate what should stay separate.
The risk isn't catastrophic PI data loss. It's quiet reconciliation errors — a lien payment posted against the wrong case, attorney reporting that looks off, documentation pulls that pull the wrong file.
For practices with active PI caseloads, a case-level review before the migration is the protective step. Knowing which patient ledgers are most complex means knowing which ones need verification first in the new environment.
Practices carrying heavy PI caseloads benefit from ChiroTouch Cloud specialists who've already worked the specific ledger issues — not generalist billers learning them live on your account.
Does ChiroTouch Cloud include automated denial management?
It includes denial tracking and reporting tools. That's different from denial management.
Tracking tells you a claim was denied and flags it for review. Management is everything after — reading the denial reason, pulling the documentation, writing the medical necessity argument, filing the appeal within the payer's window, following up until the claim is resolved.
No software automates that. Human judgment is what moves a denied claim to paid.
When a billing company pitches "the Cloud handles denials automatically," test it against your actual recovery rate. The gap between "tracked" and "recovered" is usually where active revenue defense either lives or goes missing.
How do I prevent revenue leakage during a ChiroTouch Server-to-Cloud switch?
A pre-migration AR inventory and a post-migration audit are the two protective steps. The goal is to make sure nothing with an active status gets reclassified as inactive in the transfer, and nothing that was being worked stops getting worked.
Specifically: export the AR aging report before the switch, document all open appeals and pending denials, snapshot the denial queue, flag all active PI cases with case-level balances. Then reconcile each of those against the new environment within 30 days.
The migration is also a natural moment to see whether the current billing operation is really recovering the complex revenue — or whether the switch is just surfacing gaps that were always there.
Many practices discover during this audit that the real question isn't Server vs. Cloud. It's whether to stay with the current setup or bring in ChiroTouch Cloud specialists who are built for the new environment.
Does the Cloud version actually reduce my denial rate?
No. The platform doesn't determine denial rate.
Payer rules, provider documentation, coding accuracy, and how the billing team responds to denials determine denial rate.
The Cloud can improve front-end scrubbing in some workflows. Regulatory updates arrive faster than on legacy Server. Those are marginal improvements to clean-claim submission.
They don't touch the claims that were going to be denied anyway — medical necessity arguments, documentation corrections, multi-step appeals.
Practices expecting the migration to fix the denial rate are treating a billing problem like a software problem. The platform sends the claim cleaner. Someone still has to work the claim that comes back unpaid. That work determines recovery — entirely independent of whether the EHR lives on your server or in the vendor's data center. Which is why ChiroTouch Cloud specialists worth talking to will never pitch the Cloud as a denial-rate fix.
What does a real billing audit look like during a ChiroTouch migration?
It's scoped to transition damage, not steady-state performance. The audit inventories what needs to carry forward — open appeals, active denials, pending documentation, PI case balances, Medicare claims awaiting AT modifier corrections — and verifies each one in the new environment within the first 30 to 60 days post-migration.
It also reviews the billing operation itself during the transition — how fast the team is moving in the new environment, which workflows slowed down, where claims are sitting longer than they used to.
That operational review is how active revenue defense stays in place during a window when most practices let their AR drift.
A real audit doesn't just check that the data transferred. It checks that the billing function kept functioning.
How does the platform choice interact with choosing a billing partner?
The platform is a tool. The partner is who works the claims.
Those are two separate decisions. Pretending they're the same is how practices end up with a new EHR and the same revenue problem.
The question worth asking: is the current billing operation — internal or external — actually recovering the complex revenue the practice generates? If the answer is no, the platform switch is a distraction from the decision that actually matters. If the answer is yes, the platform switch just needs a clean migration plan.
For practices evaluating both at once, choosing chiropractic billing software comes second. The billing partner decision comes first. The partner is what turns the software's output into collected revenue — or doesn't.
The Bottom Line on Server vs. Cloud for High-Volume Billing
For most high-volume practices in 2026, the Cloud migration is coming. If not now, then within the next vendor support cycle. Server still has real advantages at the local level — especially for PI-heavy practices leaning on legacy ledger flexibility. But the long-term direction is clear, and staying on Server indefinitely creates regulatory lag that's harder to defend every year.
That's the platform answer. It's also the less important one.
The more important decision is what happens to the billing operation during and after the switch. Submission is not billing. Getting paid is billing. No version of ChiroTouch — Server or Cloud — decides whether the complex claims get worked, the denials get appealed, the AR gets recovered. That outcome comes from who's reading the claim when the payer sends it back unpaid.
The platform sends the claim. Someone has to fight for the payment.
If your current setup isn't fighting for it, the migration won't change that. It'll just move the same problem into a newer interface. Most practices discover this during the audit, not before it.
The cleaner path is to ask the billing question before the platform question — and let the answer to the first one shape how the second one gets handled.
Migration moments reveal more about the billing operation than about the software.
A ChiroTouch switch is the rare time your practice can see its real revenue picture — not just the aging report, but which claims got worked, which got dropped, and what the gap actually costs. Skip the audit, and the platform change just moves the same unknowns into a new environment.
A practice assessment walks your current AR, your denial patterns, and your PI case handling through the lens of your specific ChiroTouch environment. It shows what the migration will protect, what it will expose, and what it won't change on its own.
Book a Call to see your billing operation in the light of the platform switch — before the switch makes the picture harder to read.
For practices weighing billing software compatibility alongside a billing partner decision, the diagnostic is the same. The operation underneath the software decides the outcome.
Cloud or Server, the claims still come back. The question is who's working them when they do.

© 2026 Bushido Billing. All Rights Reserved | Web Design by iTech Valet